
World Kidney Day 2019: Kidney Health for Everyone Everywhere
World Kidney Day (WKD), established in 2006, is an initiative to raise awareness about the health burden of kidney disease. The theme for World Kidney Day 2019 is global awareness, with a focus on disparities and inequities due to social determinants of health. The official WKD editorial by Crews et al dives deeper into this issue.

AJKD March 2019 Cover Celebrating World Kidney Day
For most clinicians reading this, losing a hyperkalemic patient with acute kidney injury due to a lack of dialysis nurses, dialysis machines, or basic laboratory testing is inconceivable. Unfortunately, for millions around the world, this is a daily reality. The reasons for this inequity in kidney care are complex and include socioeconomic, cultural, and political factors. The burden of kidney disease correlates with lower socioeconomic status as the latter is directly or indirectly responsible for many of the risk factors for kidney disease development and progression.
Dietary patterns in certain countries of the world have shifted from malnutrition and “low-caloric” intake to obesity and “nutrient-poor” diets. Environmental factors disproportionately affect certain geographic areas, as seen in the puzzling cases of Mesoamerican nephropathy. Infections and poor control of comorbidities (such as diabetes and hypertension) also portend a poorer prognosis and contribute to this inequity in low-income populations. The figure below illustrates how social determinants lead to health disparities that can result in the progression of chronic diseases including kidney disease:

Social determinants of health disparities framework. Figure 3 from Hall, AJKD, © National Kidney Foundation.
A large proportion of patients in low-income countries are never diagnosed with kidney disease because basic labs and urine studies are not widely available. Poor health literacy (unsurprisingly associated with low socioeconomic status) makes it challenging for patients to navigate the healthcare system or to successfully receive kidney transplantations. Additionally, medical care for kidney diseases can be expensive. In countries with universal healthcare, the cost of renal replacement therapy (RRT) is typically covered by public funds. However, in many countries, these costs are covered by patients or less commonly by private funds. The cost of kidney disease medications alone can be as high as 18 days of wages in low-income countries. This cost only increases as the disease progresses and RRT is required. You can see in Figure 1 from Crews et al that even basic tests like serum creatinine and quantification of urine protein are luxuries that most patients in low-income countries cannot afford:

Health care services for identification and management of chronic kidney disease by country income level. (A) Primary care (ie, basic health facilities at community levels [eg, clinics, dispensaries, and small local hospitals]). (B) Secondary/specialty care (ie, health facilities at a level higher than primary care [eg, clinics, hospitals, and academic centers]). Figure 1 from Crews et al, Kidney Medicine © WKD 2019 Steering Committee.
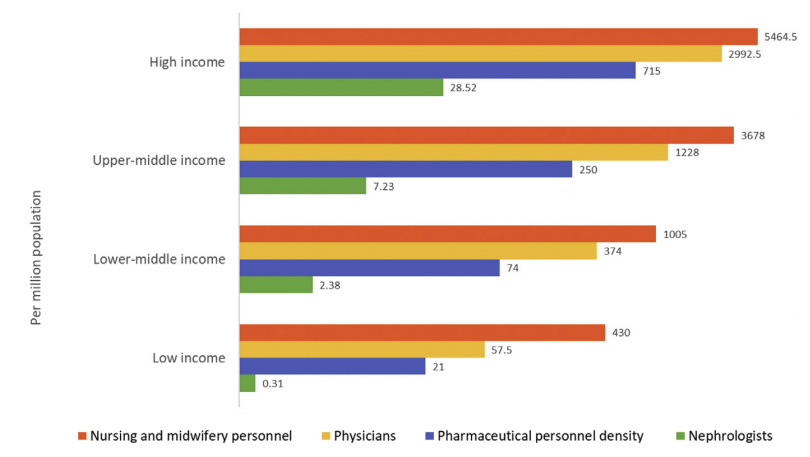
Nephrologist availability (density per million population) compared with physician, nursing, and pharmaceutical personnel availability by country income level. Figure 2 from Crews et al, Kidney Medicine © WKD 2019 Steering Committee.
Unfortunately, many of the social determinants that influence kidney disease patients in low- and middle-income countries similarly influence the United States, a high-income country. Social inequities and their link to kidney disease in the US population are the focus of a Narrative Review by Yoshio Hall published in AJKD last year. Hall describes how lack of economic stability, low levels of education, distressed and poor neighborhoods, social discrimination, and limited access to health care are important but modifiable risk factors for kidney disease progression in the US. Figure 2 in that paper shows that the social determinants of health drive 60% of premature death in the this country, with health care only being responsible for 10%:

Proportional contribution of health determinants to premature death in the United States. Figure 1 from Hall, AJKD, © National Kidney Foundation.
Importantly, Hall recommends several interventions that nephrologists can adopt to integrate health equity into clinical practice. These include:
- Collaborating on policy reforms aimed at reducing the inequities in social determinants;
- Promoting broader health insurance coverage that includes Medicaid enrollees;
- Partnering with local communities to spread awareness about kidney disease risk factors and therapies;
- Training patient navigators, health coaches, and community health workers to act as liaisons between the health system and patients;
- Screening patients for unmet social needs to improve their health and health engagements.
The mortality from kidney disease is on the rise in the US and worldwide. While there is much work to be done in the US to address social determinants of health, there may be an even bigger need to tackle these inequities in low- and middle-income countries where policies targeting kidney health may be overlooked. While the World Health Organization (WHO) has made worldwide universal health coverage one of their development goals for 2030, their action plan for the prevention and control of non-communicable diseases does not specifically include kidney disease. As a nephrology community, we should strive to place kidney disease on the global health agenda. Only then will we be able to make steps towards achieving global kidney health equity.
– Post prepared by Pascale Khairallah, AJKD Editorial Intern. Follow her @Khairallah_P.
To view the Hall Narrative Review (FREE until May 1, 2019), please visit AJKD.org.
Title: Social Determinants of Health: Addressing Unmet Needs in Nephrology
Author: Yoshio Hall
DOI: 10.1053/j.ajkd.2017.12.01
To view the Crews et al WKD Editorial (Open Access), please visit KidneyMedicineJournal.org
Title: Burden, Access, and Disparities in Kidney Disease
Author: Deidra C. Crews, Aminu K. Bello, and Gamal Saadi for the WKD Steering Committee
DOI: 10.1016/j.xkme.2019.01.002
In celebration of National Kidney Month and World Kidney Day, AJKD presents a special collection of articles highlighting various types of disparities that impact patients with kidney diseases. All articles in this collection will be freely available until May 1, 2019.


Copyright: lassedesignen / Shutterstock.com
Bonus Content: Check out the Disparities in Nephrology Region from NephMadness 2017!
Leave a Reply