
#NephMadness 2019: The Saturated Sixteen
We’ve enjoyed seeing all the photos of NephMadnessParties but now it’s time to review the results! The first round results of NephMadness 2019 are in! Check out the Current Standings to see whether your picks aligned with the votes of the Blue Ribbon Panel. Celebrate or commiserate with hashtag: #Saturated16
We present the Saturated Sixteen:

Hypertension Region

US HTN Guidelines came out strong and EU HTN Guidelines shots just never fell for them leading to an easy win for the US team.
US Guidelines wins 7-2.
Comments from the BRP:
“Europeans believe in higher blood pressure values than U.S. Poor ability to shoot to target!”
“Egads, I could read each scouting report 100 times and still be confused. And thus I suspect the vote will divide based on geography (hmm, is the #BlueRibbon panel equally distributed between the US and across the pond?). A lot of people will lose their perfect bracket in the first round just because there does not appear to be a clear winner here. SPRINT makes my practice harder; the European 140/90 can be hard enough in CKD, but 130/80? Still nothing good comes easily. US Guidelines 5.5 to 4.5 for European Guidelines.”
“Please keep it simple, easier for patients as well as healthcare staff. Amazing that there’s still such a dichotomy in opinion…”
“Let’s address elevated BPs early and often!”
“Not just patriotism here. The strong acknowledgement of the SPRINT trial is important.”
Hyperaldo Diagnosis took an early lead and despite strong defense by Hyperaldo Treatment team Diagnosis took the win.
Hyperaldo Diagnosis wins 6-3.
Comments from the BRP:
“We should just put spironolactone in the water!”
“Just the “REE-nin, not RENN-in” mandate is enough to want Dx to win over Rx. But honestly, nephrologists are detectives and pathway nerds. I shudder to think how many hyperaldo patients i may have missed, (or not). But this topic never ceases to challenge me. Hyperaldo Dx 8 to 2 over Rx”
“If possible, treat the patient not the condition. Going straight to surgery without understanding what’s up seems a little … rash…”
“We know how to find it, but how should we treat it?”
“How can you shoot if you don’t know what the goal is?”
Exercise Region

Athletes with Kidney Transplant looked a bit like a high school team out playing an NBA team, Athletes on Dialysis had an easy victory.
Athletes on Dialysis wins 8-1.
Comments from the BRP:
“Tough decision here, both seem unlikely to impact a lot of patients. Perhaps we just need a real ESRD culture change. I realize that exercising on RRT is a pipe dream for many, but I think it has a greater impact on their life than an exercising Tx patient. Dialysis 6 to 4 over transplant.”
“A bit of focus here to show up the benefits of exercise for those on dialysis would be great, and maybe help to overcome some of the barriers like staff time and confidence in supporting an exercise program. Maddy has heroically shown what can be done, though she is unique.”
“Exercise is hard for everyone but for the chronically fatigued, muscle-wasting dialysis patient almost impossible to fathom. They need the data the most.”
Exercise-Associated Nephrotoxicity and Substance-Associated Nephrotoxicity fought a hard close battle going in to double overtime but team Substance sunk a 3 pointer at the buzzer leading to a 1 point victory.
Substance Nephrotoxicity wins 5-4.
Comments from the BRP:
“There is an epidemic!”
“Great topic here! Lots of “cool” diseases. Going in I figured this was rhabdo v anabolic steroids, but there was much more to the topic. Exercise-induced renal disease (rhabdo) cases can be the worst reversible AKI I have seen, they are aberrancies. I wonder how many of them have a genetic basis for it? I’m glad the scouting report stressed this. But marathon-associated hyponatremia is such a fascinating disorder that goes into the core of me as a nephrologist. That makes it Exercise 7 to Substance 3.”
“Once again, showing up how common harm is may aid encouragement for more to participate in exercise, and aid better diagnosis of underlying conditions.”
“How many people drive themselves so hard that they get AKI? Few. How many people try stuff to get that six pack? Probably many more than we know.”
Hospitalist Nephrology Region
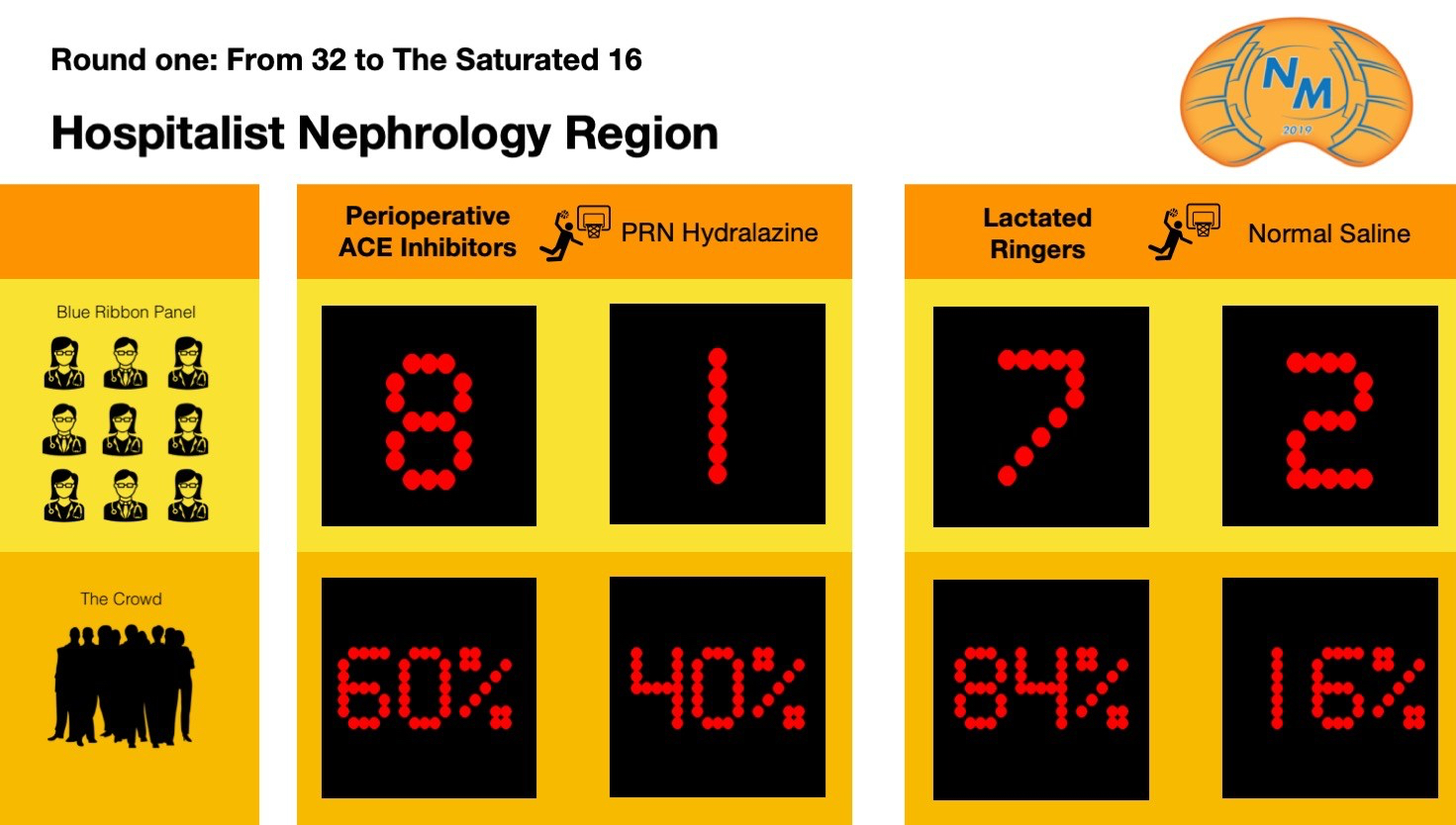
This game was all Perioperative ACE-i, Not sure that PRN Hydralazine even got off the bus, team ACE-i with the easy win.
Perioperative ACE-i wins 8-1.
Comments from the BRP:
“ACE the game!”
“Not being the person (a Hospitalist is a rich intern) that gets called for BPs at all hours I have the luxury of saying how much I hate PRN HTN medication orders. And being the person that believes RAAS inhibitors should be in the water, I think Perioperative is a much better topic. ACE-i 7 to 3 over Hydralazine.”
“We do indeed need better answers for patients – please.”
“It just doesn’t feel right to jeopardize renal hemodynamics during surgery, so, yeah, stop it. And how many of us give PRN hydralazine because we get called constantly in the middle of the night for high blood pressures?”
Despite Normal Saline’s salty defensive style, Lactated Ringers couldn’t miss a shot and had the easy win.
Lactated Ringers wins 7-2.
Comments from the BRP:
“The absolute risk difference was so small-going to be a tight game”
“Although I worry that chloride may be evil, I do relish the “normal saline ceremony” proposed by Goldfarb (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2911451/)”
“The positive effects of LR over NS are meager, but the p value is very strong because the n is so high. That is what a properly powered study does, but you cannot overlook that the differences are still meager. Regardless, why not just use RL? Putting the “Stewart” approach in the discussion was just plain mean. I’ll never understand it. LR 6 to 4 over NS.”
“Actually, it’s flip a coin for me except a very few situations.”
Pain Region

The free throw line made all the difference in this match up. Opioids couldn’t miss a free throw and NSAIDs got in to foul trouble early leading many free throws, team Opioids with the win.
Opioids wins 7-2.
Comments from the BRP:
“The new killer.”
“Good topic. Tough topic. How do you vote here: the more common topic or the unappreciated underdog? Opioids are the pariah of medicine and the media. The ‘Opioid Crisis’ is not hype. And not a week goes by that I don’t see delirium from some narcotic in a hospitalized ESRD patient. These mental status-altering metabolites are not typically removed with dialysis. You wait it out while the patient has complications. But there is no excuse for lack of pain control, unless it… I wish I knew the answer. NSAIDs have been taboo in CKD, but the risks have been exaggerated, and when you weigh the pros and cons of each…I changed my vote 3 times on this one before submitting: NSAIDs 5.5 to 4.5 over Opioids.”
“Kidney patients can lose out both ways – receiving less pain relief as some clinicians may be reluctant to prescribe or becoming addicted and harmed by opioids. I’m voting this one up to bring out more of this.”
“I love good kidney function. Giving someone a small dose of opioid for a limited time is acceptable.”
Tramadol came out and dominated the first half but a strong second half by GABAnergics led to a 2-point victory for team GABA.
GABAnergics wins 5-4.
Comments from the BRP:
“Tramadol is a heavy hitter that comes from behind.”
“This is easy. Gabapentin is the bane of my existence on the wards. Gaba 8 to 2 over Tramadol.”
“Recent patient commentary on how messy these meds can be, and hard to get on with, means it could be worth a shot this year.”
“I have seen sufficient altered mental status on all of the GABAnergics.”
Volume Assessment Region
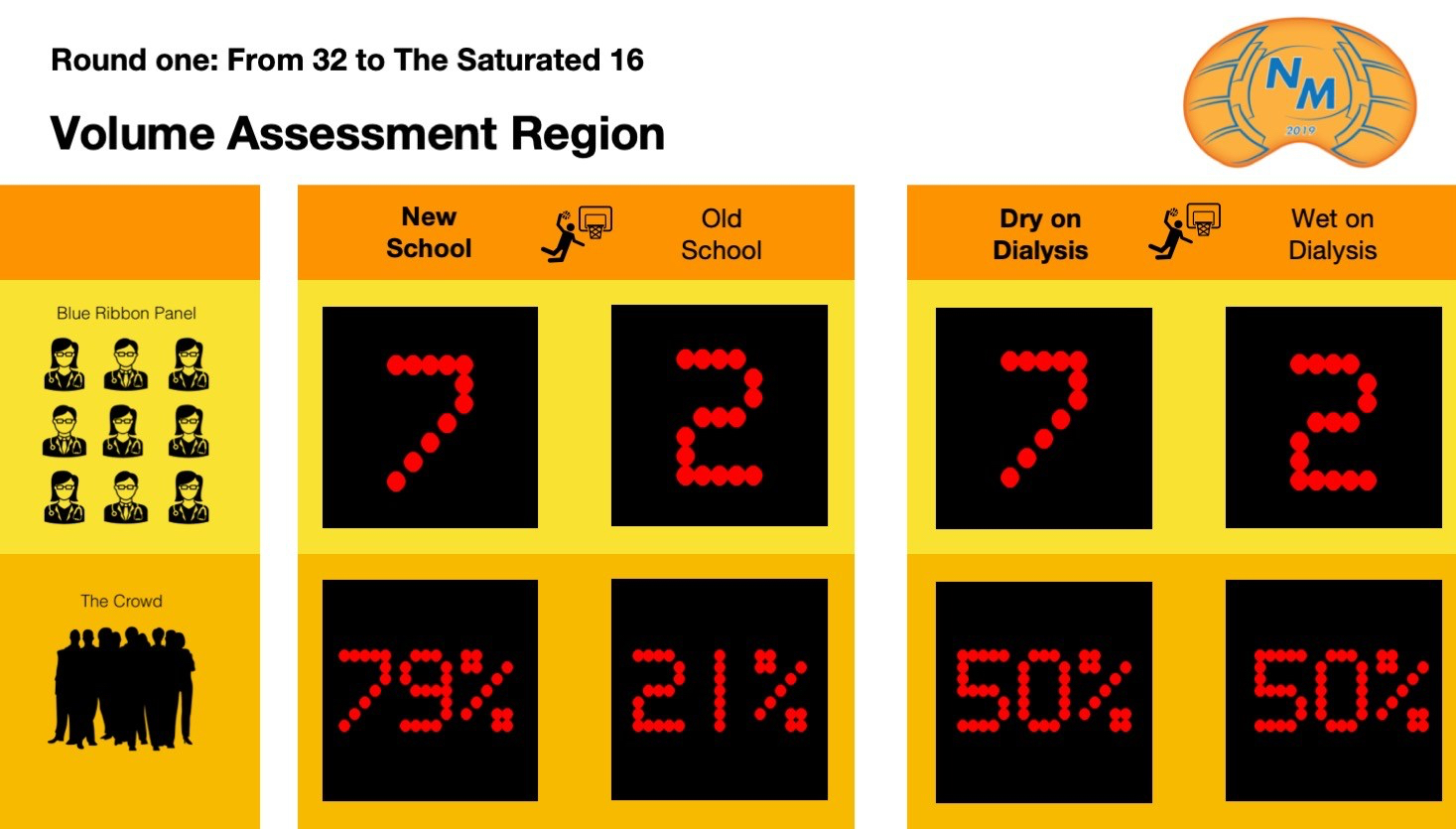
Old School could not keep up with New School’s fast past offense and strong defense. Easy win for New School.
New School wins 7-2.
Comments from the BRP:
“Old school volume management is pathetic in this department, while it may work it is so unsophisticated. Most of the newer technology seems like the emperor’s new clothes at this point, except lung US. That seems like the real deal. New school 8 to 2 over Old school.”
“Some innovation on the ‘guess my fluid’ dialysis prescription has been really welcomed by patients, especially those who have spent time having tough dialysis with poor under or over-estimates of fluid status.”
“Out with the ‘old’ and in with the ‘new’.”
“I still over dry people or throw them into pulmonary edema accidentally. We need better tools to assess volume.”
Dry on Dialysis dominated the game and team Wet on Dialysis’ shots just weren’t falling for them tonight, easy victory for team Dry.
Dry on Dialysis wins 7-2.
Comments from the BRP:
“The DRIP trial says it all.”
“Volume is the new Uremia, the new KT/V. Dry 8 to 2 over Wet.”
“Learning to value those PROMs in this most demanding of treatment is vital.”
“This is actually a hard one for me. A significant number of people seem to feel better a little wet but the data seem to indicate better outcomes if volume control is better. What the patient feels is important.”
Hepatorenal Region
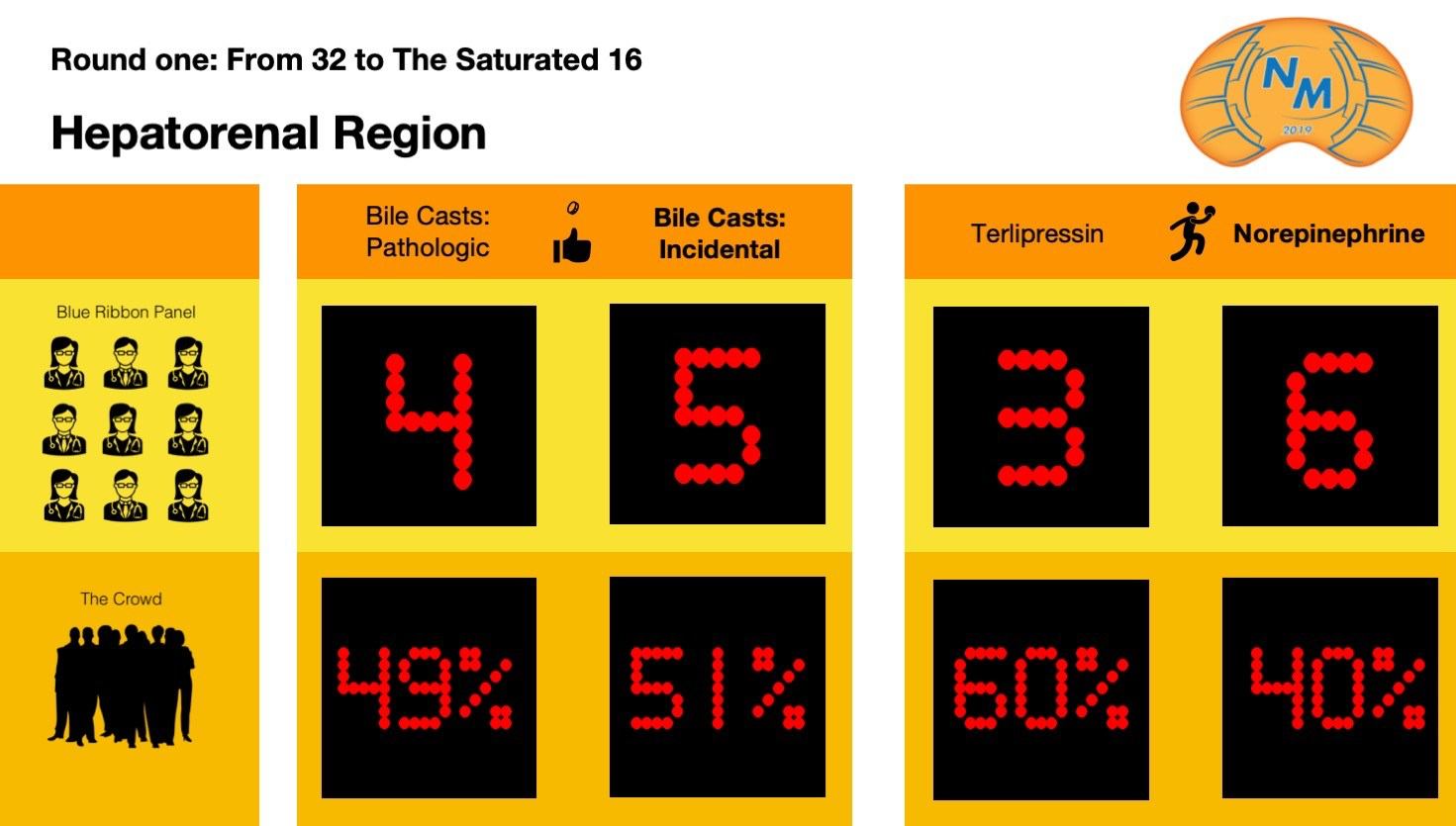
Bile Casts:Incidental and Bile Casts: Pathologic played a close game, but a last minute layup by team Pathologic led to the victory.
Bile Casts: Incidental wins 5-4.
Comments from the BRP:
“Tight race and too close to call.”
“Bile casts, myoglobin casts, Light chain casts, vancomycin casts, these could all be the effect of the AKI, not the cause of the AKI. This is very hard to tweak out the answer, but I’m more convinced for bile that they are not the cause but the effect. Incidental 7 to 3 over Pathologic.”
“The urine should be yellow, not the kidney.”
Despite the hype going into the big dance for Terlipressin, Norepinephrine came up with the easy win.
Norepinephrine wins 6-3.
Comments from the BRP:
“Norepinephrine gets down to the basics of the game.”
“I am not impressed with what we call at our institution the ‘HRS cocktail’: albumin, octrotide, and midodrine. HRS is very interesting physiology (so much more so than Cardiorenal syndrome…ugh) I wish I had more (any) experience with both agents for HRS, but I gotta go with Juan Carlos here: Norepi 6 to 4 over Terlipressin.”
“It’s a coin toss. Maybe they actually need a fecal transplant with beneficial microbiome composition.”
Plasma Exchange Region
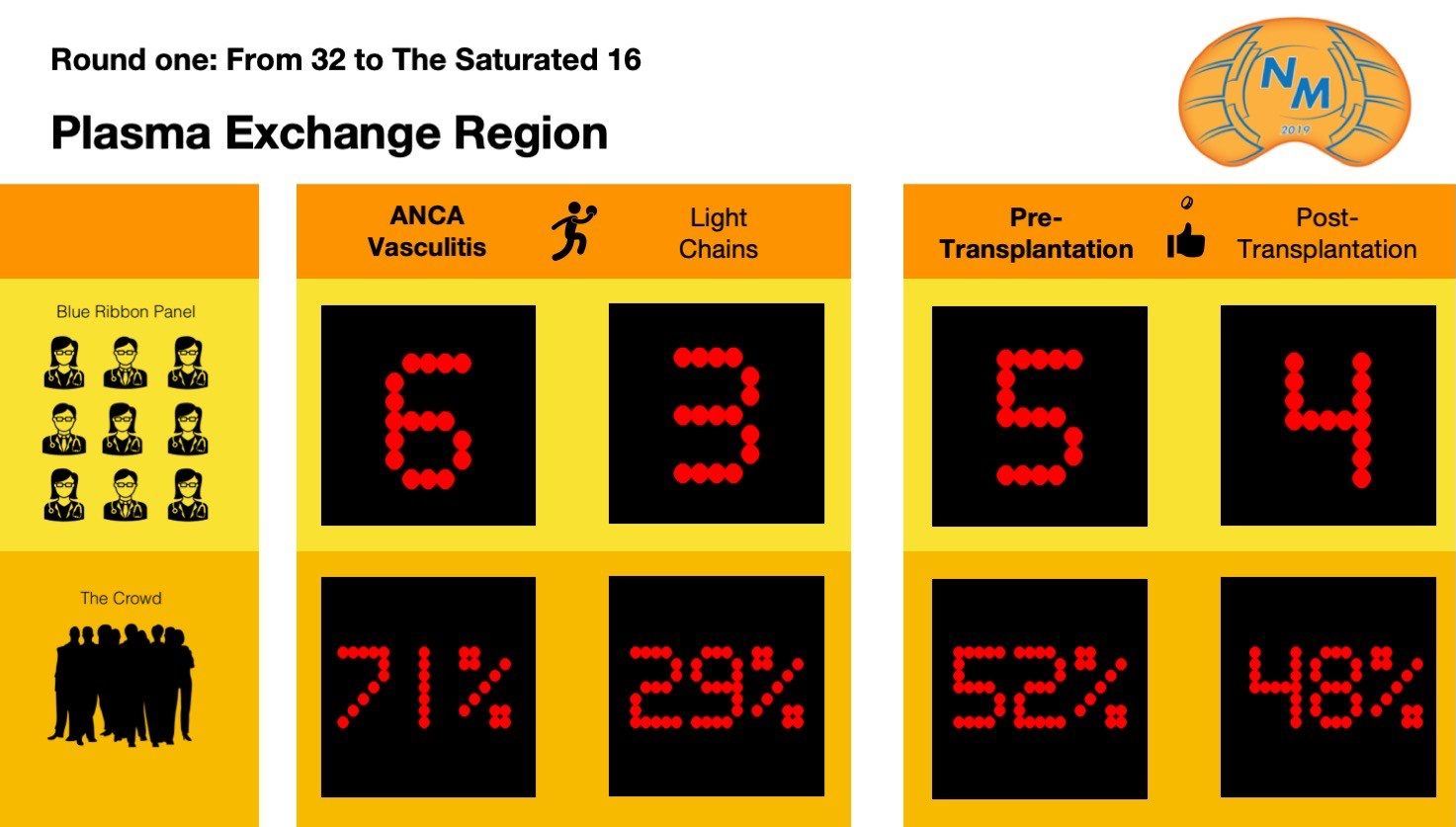
Light Chains came out and played to win but they just couldn’t keep up with ANCA Vasculitis gritty style. Team ANCA with the easy win.
ANCA Vasculitis wins 6-3.
Comments from the BRP:
“Light chains are always surprising”
“I so wanted PLEX to work for monoclonal gammopathy induced AKI and Vasculitis, but the data does not support its use in either. If the jury is still a little bit out on either (both diseases have unpublished papers on important studies still pending) I think it favors light chain PLEX. Light Chains 7 to 3 over Vasculitis.”
“The hint of reducing time on dialysis is why I have made this choice.”
“These are such uncommon diseases that our evidence-based data are too limited to feel really comfortable; however, our meds to treat vasculitis tend to work somewhat more slowly than those to treat light chains. I’ll go with the vasculitis.”
Post-Transplantation seemed likely to win the battle against Pre-transplant, but team Pretransplant came out and showed their grit and determination and pulled out the ‘W’.
Pretransplant wins 5-4.
Comments from the BRP:
“Pretransplant gets you ready for the game.”
“An ounce of prevention is worth a pound of cure. Pre 7 to 3 over Post.”
“Bring out the novel treatments to address the devastating effects of transplant rejection.”
“Too many people are forced to wait too long for a kidney due to sensitization.”
Complement Region

In the matchup between Acquired C3GN and Genetic C3GN, Acquired pulls off a narrow win over Genetic.
Acquired C3GN wins 5-4.
Comments from the BRP:
“Another tight race.”
“Forgive my irresponsibility here, but I gave up on understanding the complement system as it has evolved since I was in Medical School. I’m not convinced that acquired C3GN isn’t just genetic C3GN with a second hit. A toss-up here but I find the acquired C3GN cases more interesting. Acquired 6 to 4 over Genetic.”
“Under-recognized. We still don’t know the breadth of diseases due to genetic diseases of complement.”
Another close matchup pits Eculizumab vs C3-i and Beyond, but team C3-i managed to squeeze through to the next round.
C3-i and Beyond wins 5-4.
Comments from the BRP:
“My new favorite but have never seen eculizumab play.”
“Buzz Lightyear: “To infinity and Beyond,” kinda like “I’ll give it 110%”, but one is a joke and the other, is. well just the other. That has nothing to do with my voting. Complement is involved in many processes not typically thought to be complement-mediated. If eculizumab were cheaper and easier to get, I suspect we would be using it more like rituximab. I’m living in the present here. Eculizumab 8 to 2 over C3-i and beyond.”
“For families affected by these conditions, more research using these drugs is needed to extend the availability of transplants to them.”
“Expensive but effective.”
Current Standings | NephMadness 2019 | #NephMadness | #Saturated16 
“team Exercise sunk a 3 pointer at the buzzer leading to a 1 point victory” — I think you mean “team Substance?”
Thanks for letting us know! Post has been updated with correction.