
Don’t Panic: Pregnancy in Kidney Disease
Women of reproductive age with chronic kidney disease (CKD) who desire to have children face potential complications during pregnancy. Today we will use a recent AJKD perspective, “Women’s Reproductive Health for the Nephrologist,” in addition to other data, to walk you through a fictional scenario. In doing so, we hope to convince you that there is no need to panic in the setting of pre-conception counseling and pregnancy and kidney disease!
Case: A 22-year-old female with a history of post-streptococcal glomerulonephritis with resultant CKD stage 3 with a baseline estimated glomerular filtration rate (eGFR) of 45 mL/min/1.73 m2 and hypertension comes for follow-up. Her blood pressure is well controlled on lisinopril and she has approximately 1 gram of proteinuria. She would like to start a family in the next 2 years. How do you approach contraception in a patient with CKD? What special considerations should a nephrologist have in women of childbearing age?
There are many options for contraception in kidney disease including barrier methods, hormone-based contraceptives, intrauterine devices (IUDs), and sterilization. When counseling patients on their options, it is important to consider side effect profile, efficacy, the patient’s underlying disease, and the patient’s preference. For example, sterilization is not a viable option for this patient as she desires a future pregnancy.
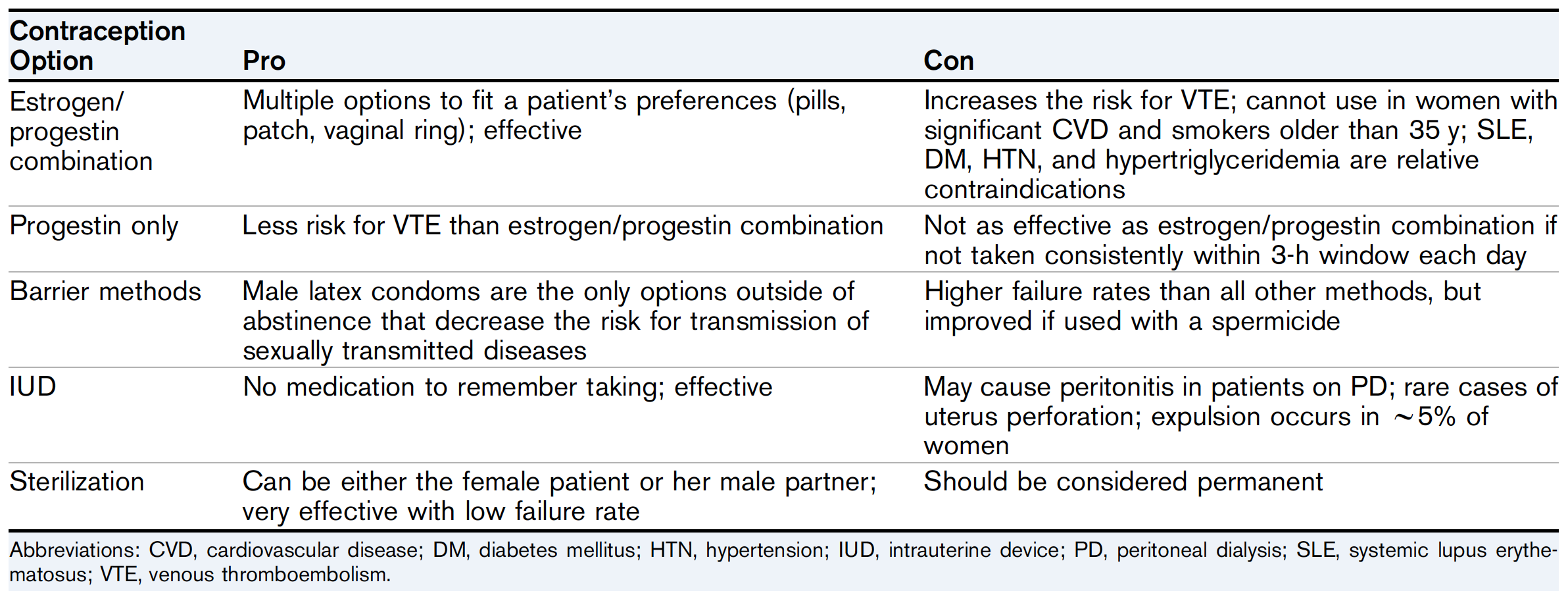
Summary of Pros and Cons of Different Contraception Choices. Table 1 from Burgner and Hladunewich, AJKD © National Kidney Foundation.
The effectiveness of various contraception options is summarized below (from the CDC):
| Contraception Option | Efficacy with Typical Use |
| Estrogen/progestin combination | 93% |
| Progestin only | 93% |
| Barrier methods | 87% |
| Intrauterine device (IUD) | 99% |
| Sterilization | 99.9% |
Nephrologists also frequently prescribe medications with potential teratogenic effects. In this case, the patient is on lisinopril for her hypertension and ongoing proteinuria. The patient should be counseled on its potential teratogenicity as well as need to use ongoing contraception while taking this medication. In addition to renin angiotensin-aldosterone system inhibitors, other common medications with potential teratogenic effects prescribed by nephrologists include mycophenolate mofetil, cyclophosphamide, and rituximab.
Your patient returns for follow-up 2 years later and her CKD has progressed to stage 4. How does kidney physiology change during pregnancy? What are the risks of pregnancy-related complications in the patient with CKD and how do they compare to the general population? What are some ways to mitigate such risks?
During pregnancy, several physiological changes occur that affect the kidneys. First, nearly all women develop hydronephrosis of the right kidney related to uterus compression and high levels of progesterone, although this does not typically affect kidney function. Progesterone also increases renal plasma flow and GFR. There is also an increase of blood volume by up to 50% and an up-regulation of the renin-angiotensin-aldosterone system which can have significant implications in the CKD population, including worsening hypertension and proteinuria as well as progression of native disease.

Image from Pixabay / gdakaska
The major complications facing patients with CKD during pregnancy include an increased risk of pre-eclampsia, pre-term delivery, intrauterine growth restriction and stillbirth. With decreasing GFR, patients are at an increased risk of both adverse maternal and fetal outcomes. In addition, in this patient, given her low GFR and ongoing proteinuria, she is at risk for faster decline of her residual kidney function.
Ideally, patients should be medically optimized prior to becoming pregnant. This includes good blood sugar and blood pressure control in patients with diabetes and at least 6 months of quiescence of lupus nephritis. Younger women with CKD 4-5 and deteriorating kidney function should consider waiting till post kidney transplant to conceive. Teratogenic medications such as angiotensin-converting-enzyme (ACE) inhibitors should be switched in preparation for pregnancy.
Patients on dialysis require 36 hours of dialysis per week during pregnancy. It is optimal for patients with end-stage kidney disease to undergo transplant prior to pregnancy if possible.
The patient and her nephrologist discuss the risks of pregnancy with her current degree of kidney disfunction and the patient decides to wait to become pregnant until she undergoes kidney transplantation. What is the ideal timing of pregnancy post-transplant? How has the risk of pregnancy-related complications changed in the setting of transplant?
Current guidelines for kidney transplant recipients suggest that woman should wait until at least one year following transplant and have had no episodes of rejection within the past year, a creatinine level ≤ 1.5 mg/dL, minimal proteinuria, no infections that could affect the fetus such as cytomegalovirus, and pregnancy safe immunosuppression. There are more recent data that shows waiting at least three years decreases risks further, particularly the risk of graft loss. Post-transplant, patients remain at an increased risk of preterm delivery, intrauterine growth restriction, and pre-eclampsia, albeit the risks are improved from stage 4-5 CKD.

Summary of Pregnancy Counseling by CKD Stage. Table 2 from Burgner and Hladunewich, AJKD © National Kidney Foundation.
Conclusion
As succinctly put in the Perspective: “It is the obligation of every nephrologist caring for women of reproductive age to provide guidance in the choice of methods to prevent unplanned pregnancies, to choose treatments that preserve fertility, and to participate in shared decision making that optimizes pregnancy timing and outcomes.” In that line of thought, we hope that you are now persuaded that there is no need to panic when it comes to reproductive counseling and pregnancy in CKD; you should now be ready to enter the conversation with your patients.
– Post prepared by Christin Giordano @CGiordano1225, AJKDBlog Guest Contributor, and Anna Burgner @anna_burgner, AJKDBlog Contributor.
To view this Perspective (FREE until Feb 29, 2020), please visit AJKD.org.
Title: Women’s Reproductive Health for the Nephrologist
Authors: Anna Burgner and Michelle A. Hladunewich
DOI: Women’s Reproductive Health for the Nephrologist
Leave a Reply