
#PathPointer: Concurrent anti-GBM disease and Membranous Nephropathy
The double positivity of Anti-Neutrophil Cytoplasmic Antibody (ANCA) vasculitis and anti-glomerular basement membrane (anti-GBM) disease is well known and well described, with 30% of patients with anti-GBM disease also testing positive for serum ANCA. A lesser known co-existence is that of anti-GBM nephritis and membranous nephropathy with subepithelial or intramembranous deposits. This combination was first described in 1976 in a 20 year old patient who presented with rapidly progressive glomerulonephritis, pulmonary hemorrhage, high titers of antiglomerular basement membrane antibodies, and a kidney biopsy that showed linear IgG staining. Interestingly, the patient had a rapid recovery of symptoms without requiring treatment, but urine sediment showed persistent hematuria and proteinuria a year later. A repeat kidney biopsy showed nonlinear IgG immunofluorescence with electron dense deposits on the subepithelial surface of the GBM.
Animal studies theorize multiple autoimmune responses to create this “double lesion,” with one disease process potentially triggering the second. These include unique target antigens within the COL4A3 chain of type IV collagen allowing for the formation of in-situ subepithelial immune complexes, rearrangement of the subepithelial immune complexes to form complex lattices, or epitope spreading. Until now, the literature on this consisted of case reports, but a recent AJKD case series from Ahmad et al describes the clinical outcomes of this rare disease.
Twelve patients were included, all of whom had linear IgG staining AND epimembranous electron-dense immune deposits on biopsy. All 11 patients who were tested had significant tiers of anti-GBM antibodies, but only 1 of the 5 tested for PLA2R on biopsy was positive. A representative kidney biopsy of one of these patients is shown below in Figure 2 from the paper.
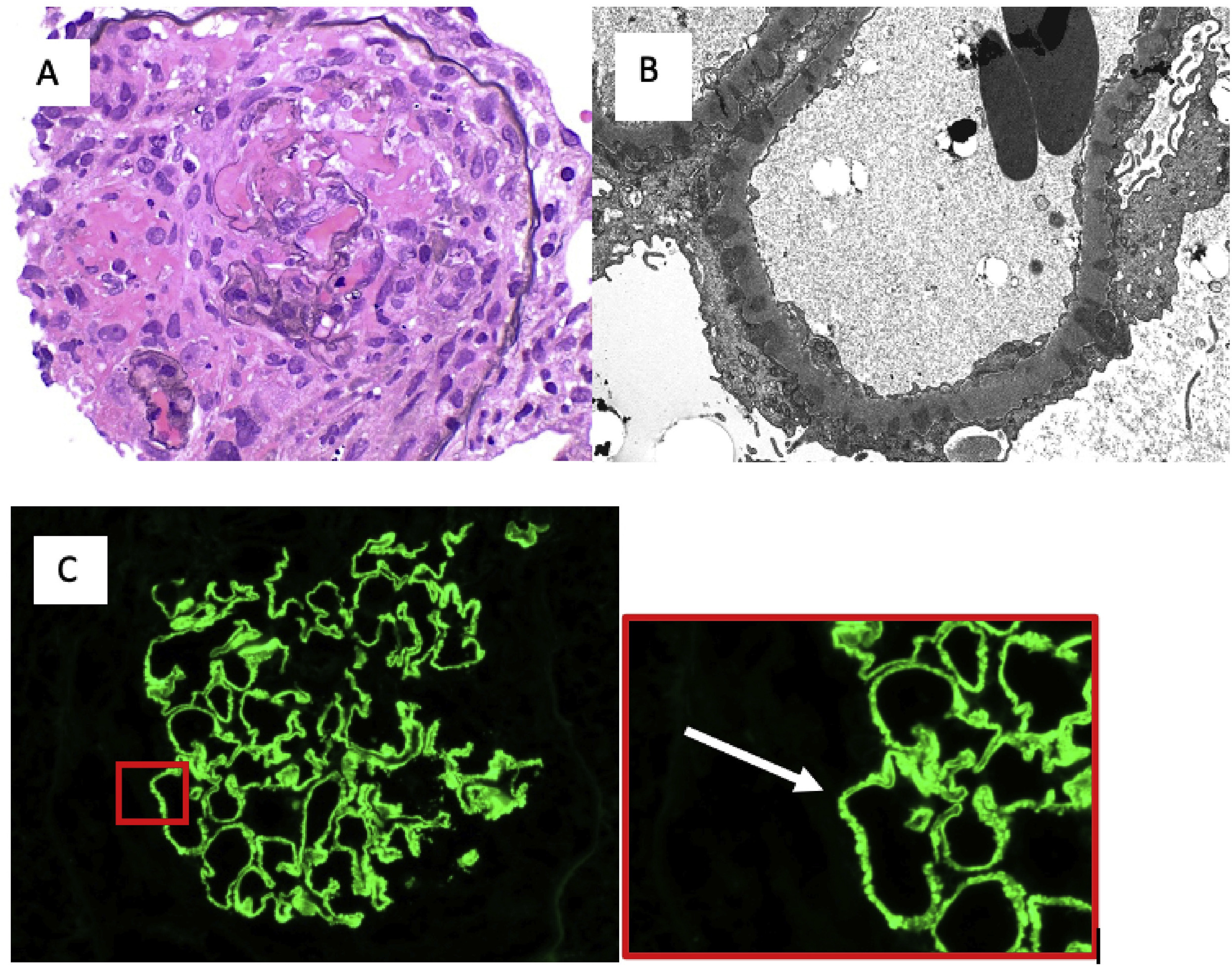
Figure 2 from Ahmad et al, AJKD © National Kidney Foundation
Kidney biopsy of case 12. (A) Representative glomerulus shows circumferential cellular crescents that disrupt Bowman capsule, associated with fibrinoid necrosis of the underlying tuft. (B) Electron microscopy revealed global subepithelial immune deposits with intervening GBM spikes. There were no mesangial or subendothelial deposits. There was 90% foot-process effacement. (C) Immunofluorescence for immunoglobulin G with 2+ linear and 1+ granular global fluorescence. Arrow indicates magnified section of immunofluorescence showing granular pattern.
The patients in this case series presented with very advanced kidney disease, with a mean serum creatinine of 9.3 mg/dL, hematuria, and sub-nephrotic range proteinuria. Only one patient had pulmonary hemorrhage. Unfortunately, all patients required dialysis shortly after presentation. The remainder of their clinical characteristics are shown below

Table 1 from Ahmad et al, AJKD © National Kidney Foundation
Treatment protocols were quite variable, with patients receiving a smattering of corticosteroids, cyclophosphamide, plasmapheresis, or rituximab. Only 2 patients had recovery of kidney function, with 7 remaining on dialysis and 3 eventually receiving kidney transplant.
Although a very limited sample, this case series provides valuable insights. Whereas concurrent anti-GBM disease and ANCA-associated glomerulonephritis has a better response to therapy, the co-existence of membranous nephropathy in anti-GBM disease portends a less favorable prognosis. It is difficult to draw conclusions from such a small number, and given the markedly reduced kidney function on presentation in this case series, the outcomes seen here were not much different from what could be expected in pure anti-GBM disease. However, this article highlights the association of these 2 rare histologic findings and demonstrates the need for aggressive therapy and future study.
– Post prepared by Timothy Yau, AJKD Social Media Editor. Follow him @Maximal_Change.
To view Ahmad et al (subscription required), please visit AJKD.org.
Title: Concurrent Anti–Glomerular Basement Membrane Antibody Disease and Membranous Nephropathy: A Case Series
Author: Syeda B. Ahmad, Dominick Santoriello, Pietro Canetta, Andrew S. Bomback, Vivette D. D’Agati, Glen Markowitz, Wooin Ahn, Jai Radhakrishnan, Gerald B. Appel
DOI: 10.1053/j.ajkd.2020.11.023
Leave a Reply