A 70-year-old woman was diagnosed with Sjögren syndrome four years ago. She also has a history of hypertension, which has recently become difficult to control. She presented with shortness of breath and was found to have pericardial effusion and a serum creatinine of 2.0 mg/dL (eGFR, 25 mL/min), elevated from baseline of 1.0 mg/dL (eGFR, 55 ml/min). Urinalysis showed microscopic hematuria with 5-10 RBCs/HPF. Urine protein/creatinine ratio was 2.5 g/g. Laboratory workup revealed an ANA of 1:2560, but dsDNA was negative. Serum C3 was low at 61 mg/dL, and C4 was unmeasurable. Rheumatoid factor was high at 400 IU/mL. ANCA test was negative. Liver function tests were normal. Serum calcium was 7.8 mg/dL. Hepatitis B and C virus serologies were negative. She weighed 170 pounds with a BMI of 30. A kidney biopsy was performed.
1 / 7
What is the most likely diagnosis?
Diffuse proliferative lupus nephritis with lupus vasculitis.
Incorrect Diagnosis: Although the patient had high ANA titers, the absence of widespread glomerular immune complex deposition, the undetectable serum C4 with only mildly decreased serum C3 levels, and the absence of endothelial tubuloreticular inclusions make proliferative lupus nephritis with lupus vasculitis unlikely.
Cryoglobulinemic glomerulonephritis and vasculitis.
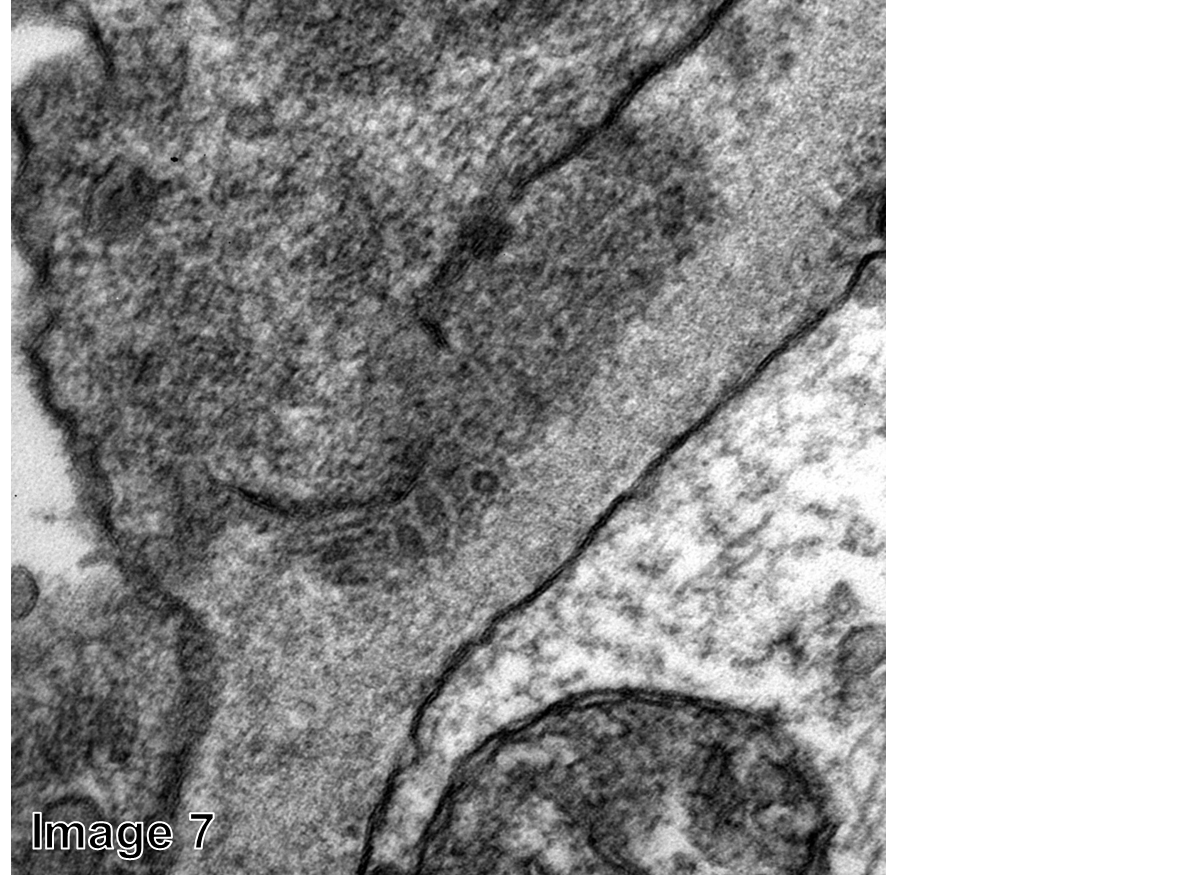
Correct Diagnosis: The paraffin sections for light microscopy contained renal cortex with 19 glomeruli; only one of which was obsolescent. The remaining glomeruli were hypercellular with some lobular accentuation (Image 1). Glomerular necrosis/crescent formation was not seen. Glomerular capillary hyaline thrombi were not present. Sections contained a small interlobular artery with transmural inflammatory cell infiltrate (Image 2). In addition to infiltrating inflammatory cells, deposition of homogeneous eosinophilic material was noted in the vascular wall (Image 3). There was evidence of acute tubular injury as well as some patchy interstitial mononuclear cell infiltrate, which contained predominantly CD3 and CD5-positive T cells admixed with some CD20-positive B cells. The interstitial fibrosis was mild and patchy. Frozen sections cut for immunofluorescence contained four hypercellular glomeruli. The reaction with the antibody to IgG showed scattered positive granules in the mesangium and along the glomerular capillary loops (Image 4). Similar granular, somewhat segmental paramesangial and glomerular capillary staining was noted for IgM (Image 5) as well as kappa and lambda light chains and C3. No glomerular staining was noted for IgA, C1q, fibrinogen, and albumin. Polyclonal cast staining was evident. Scattered interstitial plasma cells stained for IgG and kappa and lambda light chains. One glomerulus was available for electron microscopy. Ultrastructurally, only a few paramesangial, intramembranous, and subepithelial electron-dense deposits were identified (Image 6). On higher magnifications, some of these deposits had a microtubular substructure. The diameter of the microtubules was 24.0 +/- 5.1 nm. In addition, there was widespread mesangial cell interposition along many glomerular capillary loops. Endothelial tubuloreticular inclusions were not seen. The foot process effacement was moderate to prominent (approximately 60-70%).
This case demonstrates how difficult the diagnosis of cryoglobulinemic glomerulonephritis can sometimes be. In a typical case when numerous glomerular intracapillary hyaline thrombi are present in the setting of hepatitis C virus infection, the diagnosis is easy. These intracapillary hyaline thrombi and additional glomerular deposits stain strongly for IgG, IgM, kappa, and lambda light chains, and electron microscopy reveals microtubular substructure. In this biopsy, the deposits were scant, and, in our experience, this is not unusual in cryoglobulinemic glomerulonephritis. In fact, we usually raise the possibility of underlying cryoglobulinemia if we encounter an endocapillary proliferative glomerulonephritis with paucity of immune complex deposits. The undetectable C4 levels and the high rheumatoid factor levels are laboratory findings strongly suggestive of cryoglobulinemia. In this kidney biopsy, cryoglobulinemic vasculitis was also evident, which is mostly not seen in kideny biopsies with cryoglobulinemic glomerulonephritis. However, seeing vasculitis in a kidney biopsy is rare, even in other forms of systemic vasculitides, such as in ANCA-associated vasculitides. The cryoglobulin test is frequently false-negative; therefore, a negative cryoglobulin test does not exclude the possibility of cryoglobulinemic glomerulonephritis. Cryoglobulinemic glomerulonephritis is most frequently seen in association with hepatitis C virus infection, but Sjögren syndrome is perhaps the second most common underlying etiology. This patient had Sjögren syndrome-associated type II cryoglobulinemia with associated glomerulonephritis and vasculitis.
After the biopsy, the first cryoglobulin test was negative but the repeat test was positive. After a 4-week course of rituximab, the patient’s proteinuria decreased to 0.4 g/day and her serum creatinine decreased to 1.3 mg/dL and her eGFR rose to 42 mL/min.
Membranoproliferative glomerulonephritis.
Incorrect Diagnosis: To diagnose membranoproliferative glomerulonephritis, one has to see numerous mesangial and glomerular capillary (mainly subendothelial) immune complex deposits that stain for IgG and C3 by immunofluorescence. In membranoproliferative glomerulonephritis, the serum C3 is frequently low but the serum C4 level is usually normal.
Pauci-immune crescentic and necrotizing glomerulonephritis with microscopic polyangiitis.
Incorrect Diagnosis: Although there were only a few glomerular immune complex deposits, the findings are not consistent with pauci-immune crescentic and necrotizing glomerulonephritis because of the endocapillary hypercellularity and the absence of crescents and glomerular necrosis. Interestingly, crescent formation is rarely seen in cryoglobulinemic glomerulonephritis.
Immunotactoid glomerulonephritis.
Incorrect Diagnosis: Because of the microtubular substructure in the deposits, the possibility of immunotactoid glomerulonephritis emerges. In fact, in a broader sense, cryoglobulinemic glomerulonephritis is a form of immunotactoid glomerulonephritis because the deposits have organized substructure. Still, the strict definition of immunotactoid glomerulonephritis includes the absence of cryoglobulinemia, which this patient had.
Post prepared by and all images courtesy of Tibor Nadasdy, MD,AJKD Blog Contributor and AJKD Kidney Biopsy Teaching Case Advisory Board member.