

AJKD Blog
Official Blog of the American Journal of Kidney Diseases













Follow Blog by Email:
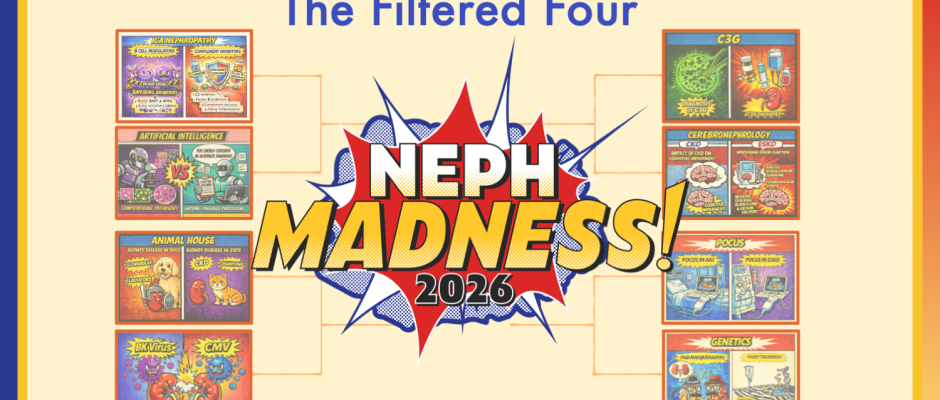
Champion Announcement
April 10, 2026
Current Standings
Check the leader board to see who is being reabsorbed and who is just metabolic waste. To Commiserate or Celebrate: #NephMadness (X) | #NephMadness (Bluesky)
NephMadness 2026 Schedule
March 1: Bracket entry opens
March 31: Bracket entry closes 11.59pm EDT
April 2: 1st round results | Effluent 8
April 6: Effluent 8 results | Filtered 4
April 8: Filtered 4 results | Finalists
April 10: NephMadness Champion crowned

Copyright © 2026 Powered by WordPress.com.