
Hyponatremia and the Brain: Ground Rules for Nephrology’s Feistiest Debate
Emmanuel Adomako @EAAdomako is currently an Assistant Professor at the University of Kansas Medical Center. He graduated from the Kwame Nkrumah University of Science and Technology in Kumasi, Ghana, where he was the editor of the medical students’ journal. He completed his internal medicine residency at the Englewood Hospital and Medical Center, Englewood, NJ. He moved to Dallas for his clinical/research nephrology fellowship at the University of Texas Southwestern Medical Center. His research interests include kidney stones and mineral metabolism. Dr Adomako is a 2023-24 AJKD Editorial Intern.
No other condition elicits as passionate a response among nephrologists as hyponatremia. If you need to be convinced, then consider the reaction to a recent retrospective review on the risk of osmotic demyelination syndrome in hyponatremia. The response to this paper can be categorized into two groups. A very simplistic and facetious description follows. On one hand, are the sodium iconoclasts, a group who hold up this retrospective paper aloft, almost as a hammer, and demand smashing down long-held restraints on the correction of hyponatremia. The opposing group is the sodium conservatives, a group defined by the constant refrain, “Stay the course.” For the latter group, there is nothing to see here.
I once heard a much wiser person say this, “Before you pull down a wall, ask why it was put up in the first place.” When thinking about hyponatremia, you begin with the brain. The human body, physiologically speaking, may not care about sodium per se. The plasma sodium concentration is the largest contributor to plasma tonicity. Defending against osmotic forces is critical for brain health. You can think of the brain like a soldier in a tank or a submarine. The tank or submarine is very protective if things go according to plan. When under attack, however, that protection could be your undoing. Protected in a bony skull, the brain does not have potential space like the subcutaneous tissue or even “third spaces” like the abdomen to tolerate edema. Similarly, brain growth outpaces growth of the skull in early life and thus older children are more at risk of poor outcomes from cerebral edema compared to adults.
Nephrologists are not morbid anatomists and so we do not open skulls to assess for changes in the brain. We rely on neurologic manifestations or if very bad outcomes (like the much-feared or much-derided central pontine myelinolysis (CPM)) ensue, then we image the brain. Most of the available evidence on the effects of hyponatremia on the brain is based on in vitro cell models, animal studies or postmortem human studies. In a recent study published in AJKD, Suarez et al attempt to answer the fundamental question of changes in the brain that occur with chronic hyponatremia.

This was a prospective cohort study conducted over four years at the emergency department of the University of Cologne, Germany. Adult patients with serum sodium <125 mmol/L who provided informed consent were recruited for the study if they were euvolemic, devoid of organic brain disease, and did not have severe symptoms like seizures or depressed consciousness on presentation. Additionally, recruited patients had to be able to undergo an MRI. Study patients underwent two sets of tests: standardized neuropsychological testing (NPT) and functional MRI. The NPT battery comprised 5 tests that assessed global cognition, mobility, and depression. The functional MRI assessed brain volume in the 3 brain compartments (white matter, grey matter, and CSF) and specific areas of the brain presumed to be structural correlates of neurologic manifestations and which were defined as regions of interest (ROI). Functional assessment comprised spontaneous brain activity and synchronized brain activity. The two sets of tests were conducted before treatment and after serum sodium > 130 mmol/L. To allow for brain adaptation, the two sets of tests were conducted at least 48 hours apart.
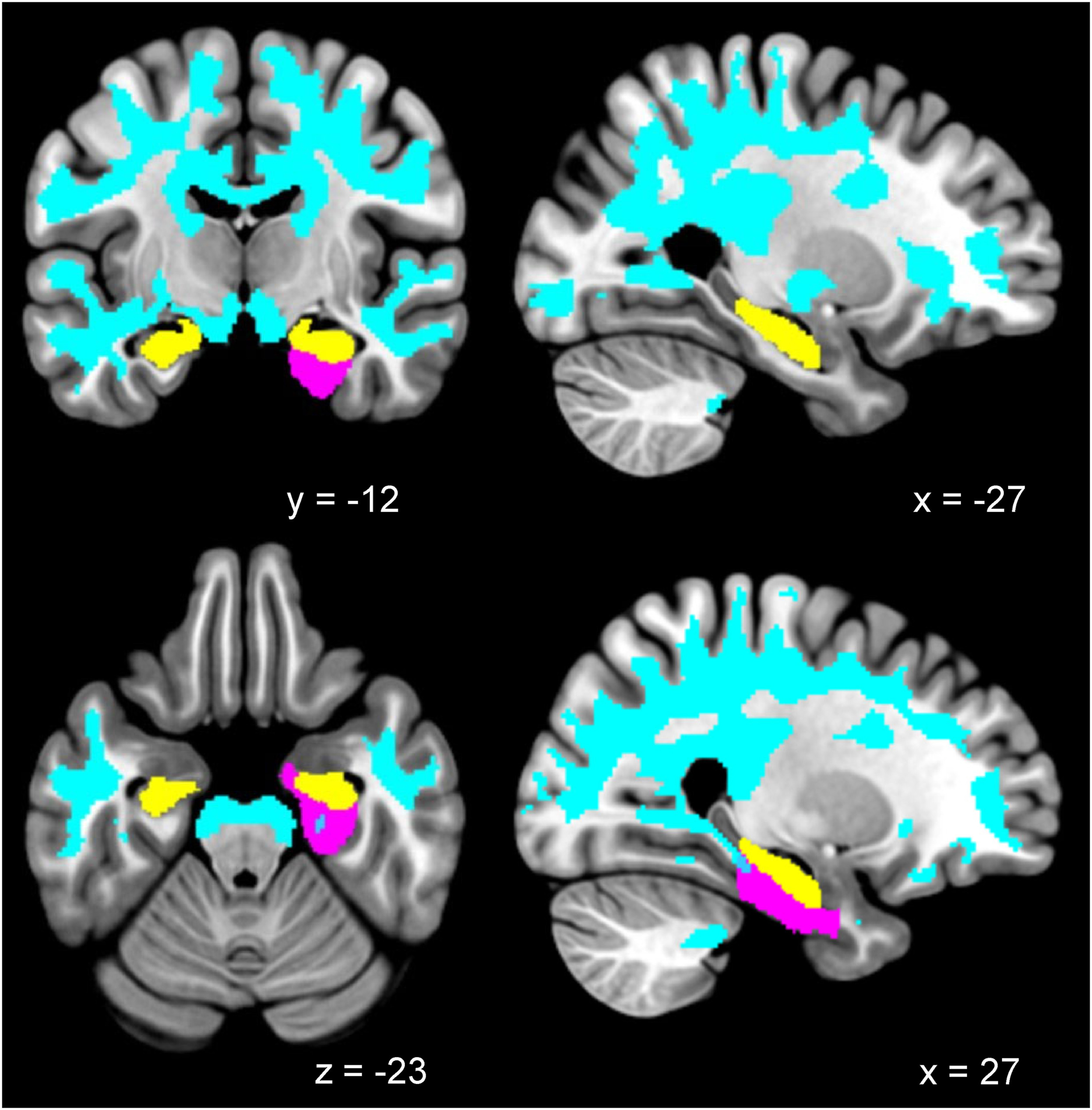
Voxel-based morphometry analysis showing clusters of greater white matter volume in session 1 (hyponatremia) than in session 2 (normonatremia; cyan color represents a threshold-free cluster enhancement–inferred, family-wise error–corrected P value lower than 0.05). Region of interest–based localization of hippocampus (yellow) and right parahippocampal and ambient gyrus (purple). Selected slices are displayed on the Montreal Neurological Institute 152 template (N = 21). Figure 1 from Suárez and Picotin et al , © The Authors.
Despite the study taking place at a large academic center in the 4th largest city in Germany, over 4 years, only 26 patients were enrolled for the study. Although the paper is silent on the number who were screened and not enrolled, it is reasonable to assume that at such a large academic center, the number of patients who presented with serum sodium <125 mmol/L would have at least been in the hundreds. The burden of the tests on patients and the need to initiate treatment may have dampened enrolment. The actual number of patients who were analyzed was reduced further by either an inability to complete the NPT or poor image quality on functional MRI. At this point, we all ought to duff off our hats to the study authors. Countless times when I have eagerly awaited an MRI report, my bubble of enthusiasm has been burst by sharp phrases like motion degraded images. Our sympathies must equally lie with the hyponatremic patients with subtle neurologic manifestations who were instructed to “let their mind wander and to keep their eyes closed to minimize eye movement.” Thus unsurprisingly, only half the recruited patients had images of sufficient quality for inclusion in the analysis. With the NPT, just over 70 percent of the patients completed the pre- and post-treatment assessments.
Having overcome the challenges inherent in such a study, what did the authors find? The first striking finding, albeit not the focus of the paper, was how long it took to correct the serum sodium and administer the second set of tests. The mean time between both sessions was close to 3 weeks (18.6 days) with a median of one week. That sounds like an awful long time to raise serum sodium from a mean of 118.4 to 135.5 mmol/L. Perhaps these physicians were of the party of sodium ultra-conservatives. The median suggests that the mean duration of 18.6 days was driven by a few outliers including the one patient who took 79 days to correct.
How does hyponatremia affect neuropsychological processing?
Except for the Timed Up and Go test (TUG), there was significant improvement in all the NPTs. With the TUG, there was a trend toward improvement without reaching statistical significance. Something to be learned here is the improvement in symptoms of depression with the successful treatment of hyponatremia. This is interesting because of the association of whole classes of antidepressants with hyponatremia. A cynic may well conclude that for makers of antidepressants, it is indeed the gift that keeps giving.
How does hyponatremia affect structure and function?
Beginning with brain structure, the study found that the volume of grey matter, white matter, and the whole brain decreased significantly whilst CSF volume increased with the normalization of sodium. When assessing specific regions of interest, volume changes were most significant in the hippocampus, right parahippocampal region, and ambient gyrus.
Neuronal activity and synchronization of neuronal activity were increased during hyponatremia. Both phenomena could underlie the noted changes in the NPT whilst the latter could lower the seizure threshold as well.
Taken together this study demonstrates that structural and functional changes in the brain which occur with hyponatremia improve with treatment. Since no premorbid structural assessments were available, the authors are at pains to stress their study does not prove that treating hyponatremia leads to the resolution of brain edema. It is nonetheless a reasonable assumption.
Back to the debate. If at this point, you are undecided as to which party you belong – sodium iconoclasts or sodium conservatives– this paper is a good place to begin. It is a wild world out there, of clever arguments and passionate pleas to sway you one way or the other and it is important to be well armed with some fundamentals underpinning the controversy.
– Post prepared by Emmanuel A. Adomako @EAAdomako
To view Suárez et al [OPEN ACCESS], please visit AJKD.org.
Title: Chronic Hyponatremia and Brain Structure and Function Before and After Treatment
Authors: Victor Suárez, Rosanne Picotin, Ronja Fassbender, Hannes Gramespacher, Stefan Haneder, Thorsten Persigehl, Polina Todorova, Matthias Johannes Hackl, Oezguer A. Onur, Nils Richter, and Volker Burst
DOI: 10.1053/j.ajkd.2023.11.007
Leave a Reply