
#NephMadness 2017: Diabetic Nephropathy Region

Copyright: Andrey Popov / Shutterstock.com
Submit your picks | NephMadness 2017 | #NephMadness or #DNRegion
Selection Committee Member for the Diabetic Nephropathy Region:
Anna Burgner
Dr. Burgner, MD, MEHP, is an assistant professor in nephrology at Vanderbilt University Medical Center in Nashville, TN, and the associate nephrology fellowship program director. She completed her internal medicine residency and nephrology fellowship at Vanderbilt. After completing her nephrology fellowship, she obtained a Master of Education in Health Professions from Johns Hopkins University. Her time is split between clinical practice, teaching medical students, residents, and fellows, and clinical research. Follow her @anna_burgner.

Competitors for the Diabetic Nephropathy Region
ACEi and ARB for Nephroprotection vs Glycemic Control
SGLT2 inhibitors vs GLP1 agonists
ACEi and ARB for Nephroprotection

Copyright: bluebay / Shutterstock.com
There are teams that have runs of greatness followed by years of rebuilding, and there are teams that are perennial powerhouses, like Duke, Kentucky, and Indiana. Then there’s Kansas. Kansas is in the midst of a 29 year streak of consecutive NCAA appearances with 6 final fours, 3 runner-ups, and a championship in 2008. This year they will break the record for the longest streak (North Carolina also had a 27 year streak from 1975-2001). Kansas has been so consistent for so long that one could call them the ACE inhibitor of basketball.
ACE inhibitors and angiotensin receptor blockers have been the reigning champs in diabetic nephropathy for over 2 decades. The critical role of the renin angiotensin system (RAS) in diabetic nephropathy has been extensively studied and well-summarized in many reviews (such as this one by Roscioni et al). Briefly, intrarenal RAS activation plays a major role in the pathogenesis and progression of diabetic nephropathy. Overall, since the importance of RAS inhibition in diabetic nephropathy was discovered there appears to be a slowing of the incidence of ESRD from diabetic nephropathy in multiple regions, including the USA, Catalonia, and Australia and New Zealand.

In type 1 DM, angiotensin-converting enzyme (ACE) inhibitors have been studied in both early and late in the course of diabetic nephropathy. Early in the course of diabetic kidney disease, when moderately increased albuminuria is the only clinical sign of a problem, captopril decreased the rate of albuminuria excretion as well as the risk of progression to overt diabetic nephropathy when compared to placebo. The Collaborative Study Group found that in subjects who already had overt diabetic nephropathy, treatment with captopril slowed the rate of GFR decline, decreased the risk of ESRD, and in some cases led to long term remission of nephrotic syndrome and preservation of kidney function.

Of the 40 patients with nephrotic range proteinuria in the Captopril study group, 8 of them had remission of the nephrotic syndrome. None of the 63 in the placebo group achieved remission. Table 1 from Wilmer et al, AJKD, © National Kidney Foundation.
In type 2 DM, angiotensin receptor blockers (ARBs) have been shown to have clear renoprotective effects in overt diabetic nephropathy. IDNT randomized 1715 subjects with hypertension and overt nephropathy to irbesartan 300 mg/day, amlodipine 10 mg/day, and placebo. At a mean follow up of 2.6 years, the group treated with irbesartan had a significantly lower risk of doubling serum creatinine or progression to ESRD than the other groups. The RENAAL trial compared losartan to placebo in 1513 subjects with overt diabetic nephropathy. Treatment with losartan reduced the risk of doubling of serum creatinine and progression to ESRD at a mean follow up of 3.4 years.


| RENAAL | IDNT | |
| Lead author | B. Brenner | E. Lewis |
| Drug | Placebo vs Losartan | Placebo vs amlodipine vs irbesartan |
| N | 1513 | 1715 |
| Median follow up | 3.4 years | 2.6 years |
| Primary outcome | composite of time to doubling of serum creatinine, ESRD or death | |
| Primary outcome | Risk reduction 16% p=0.02 | Risk reduction v placebo 20% P=0.02 Risk reduction v amlodipine 23% P=0.006 |
ACE inhibitors have also shown benefits in type 2 DM. The ADVANCE trial compared the combination of perindopril-indapamide to placebo in over 11,000 subjects with type 2 DM. The active therapy group had lower risk of new onset of moderately increased albuminuria, less worsening of moderately increased albuminuria and less new onset or worsening of severely increased albuminuria. The DETAIL trial compared the ACE inhibitor enalapril to the ARB telmisartan in subjects with early diabetic nephropathy and found that telmisartan was not inferior to enalapril in providing renoprotection.
In diabetic nephropathy, it appears there can be too much of a good thing. Last year’s NephMadness “Missteps in Nephrology Region” taught us this when it summarized the data from ACEi+ARB combo trials including VA Nephron-D, a trial where the combination of treatment with losartan and lisinopril led to a significant increase in adverse events and no improvement in mortality or slowing of CKD progression when compared to treatment with losartan alone.
ACEi or ARB are clearly indicated in the treatment of diabetic nephropathy, but are not always tolerated due to side effects of hyperkalemia or hypotension. Will this be the year that the reigning champ in diabetic nephropathy cruises through the Filtered Four to sit at the top of the dance, or will the king be dethroned?
Glycemic Control

Copyright: jarun011 / Shutterstock.com
In college basketball the players are always changing but the coaches remain the same. Some are juggernauts in all phases of the game (Mike Krzyzewski), some are incredible recruiters (John Calipari) and others are great at teaching the fundamentals. This last group is skilled at getting good players to be great. Tony Bennet, coach of the Virginia Cavaliers is that type of coach and he does it by being the best defensive coach in college basketball. Coaching fundamentals isn’t glamorous but it is the key to victory.
In diabetes there is nothing as fundamental than hyperglycemia. If one does not have DM, one cannot develop diabetic nephropathy (even though nodular glomerulosclerosis that looks like diabetic nephropathy that has been found in metabolic syndrome without overt diabetes). While type 1 DM and type 2 DM have different pathogenesis, the end result of both is hyperglycemia. Hyperglycemia has been shown to activate the intrarenal RAS system which plays an important role in the development of diabetic nephropathy. Logically, it should follow that good glycemic control is a critical part of the treatment of diabetic nephropathy. As it turns out, the efficacy depends on when this strategy is started, and the best evidence is in type 1 DM.
The landmark DCCT definitively showed the importance of early glycemic control in subjects with type 1 DM. DCCT randomized subjects to a target A1C of 7% vs 9% and included 1,365 subjects with normal albumin excretion at baseline. The remaining 73 subjects had moderately increased albuminuria. The tight glycemic control group had a significant reduction in the onset of albuminuria. The long term follow up of DCCT, the EDIC study, found that the renoprotective effects of a lower glycemic target were sustained long term. Eight years after DCCT was completed, subjects initially assigned to the intensive glycemic control group continued to have a lower risk of development of albuminuria. 16 years after DCCT was completed they were less likely to have developed impaired renal function. After the completion of the study all patients had the same therapy and the hemoglobin A1c of the two groups were indistinguishable (7.9 ±1.1 for the intensive therapy group and 8.0 ±1.0 in the conventional therapy group). Of note, the total mortality has a more complex relationship with glycemic control with a definite advantage for the conventional group. This group was weaned gradually until tighter control had the upper hand.

Patients with type 1 DM who already have moderately increased albuminuria also appear to benefit from intensive glycemic control, although the data is less definitive given its small size. The 73 subjects with moderately increased albuminuria at baseline in the DCCT had similar benefits to those without albuminuria at baseline. A meta-analysis of smaller, earlier trials also suggests benefits to intensive glycemic control in the setting of already established, moderately increased albuminuria. Once severely increased albuminuria has developed in type 1 DM, most of the data comes in the setting of multiple small studies of subjects who have become normoglycemic after receiving pancreas transplants. Pancreas transplant led to a reduction in albuminuria in one study at a year post transplant, and in another study led to improvement of biopsy findings in diabetic nephropathy at 10 years, but not at 5 years post-pancreas-transplant.
In type 2 DM the data is less concrete. The UKPDS trial found that subjects with newly diagnosed type 2 DM who were treated with intensive glucose control did not have improved renal outcomes. The ADVANCE trial found a reduced risk of albuminuria, but no reduction of the risk of doubling of serum creatinine in subjects who had type 2 DM for an average of 8 years. VADT, on the other hand, found a benefit only in tight glycemic control for the risk of progression of albuminuria from moderately increased to severely increased. Then there is the ACCORD trial, which was stopped early due to increased deaths (including increased cardiovascular deaths) in the intensive treatment arm. ACCORD used a lower target A1C for the intensive glucose control than the previously mentioned studies at <6%, suggesting (at least in type 2 DM) that overly intensive glucose lowering may increase harm. To make matters more uncertain in the treatment of type 2 DM, a meta analysis of 7 large trials including over 28,000 subjects with type 2 DM found that intensive glucose control reduced the risk for moderately and severely increased albuminuria, but unfortunately did not decrease the risk for doubling of serum creatinine, nor of renal death.
Glycemia control had a fast start to the season with its role in decreasing the risk of developing diabetic nephropathy in type 1 DM, but since then things have been rocky. Is hyperglycemia the new Baylor, with two first round exits after being seeded third and fifth the last two years?
Sodium Glucose Lumen Transporter 2 (SGLT2) inhibitors

Copyright: MoQcCa / Shutterstock.com
In 2013 Florida Gold Coast rocked the NCAA tournament. They entered the tournament as a #15 seed but they took their “Dunk City” style of play and beat #2 Georgetown on their way to being the first #15 seed ever to advance to the Sweet 16.

Copyright: xamnesiacx / Shutterstock.com
2013 was also the year canagliflozin (Invokana) was approved for sale in the United States, becoming the first of a new wave of SGLT2 inhibitors for the treatment of type 2 diabetes mellitus (DM). SGLT2 inhibitors have the beneficial effects of promoting weight loss and avoiding hypoglycemia and hyperinsulinemia. The currently available SGLT 2 inhibitors in the U.S. are:
| Canagliflozin | Invokana | 100-300 mg qd |
| dapagliflozin | Farxiga | 5-10 mg qAM |
| Empagliflozin | Jardiance | 10, 25 mg qAM |
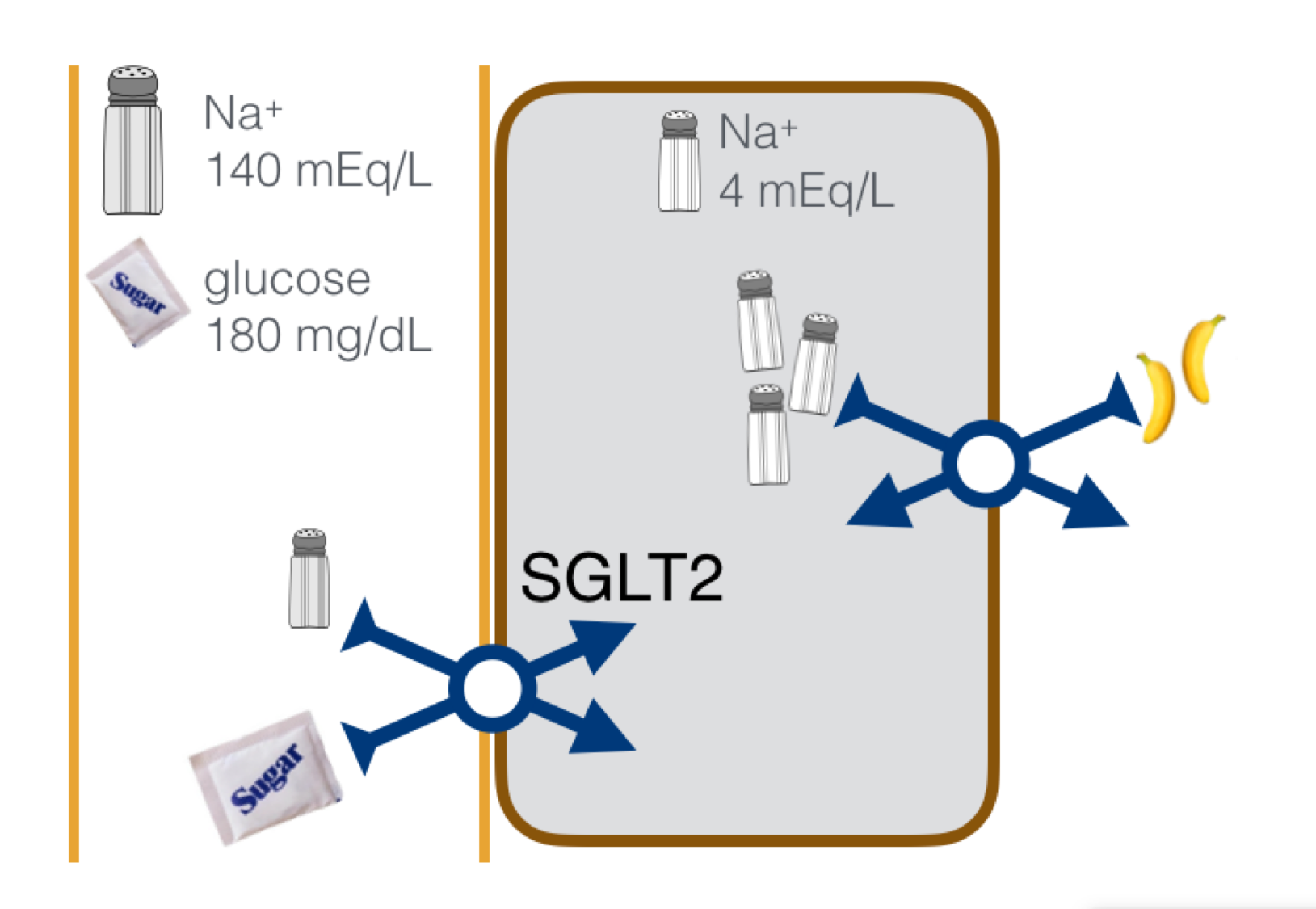
SGLT2 reabsorbs Na+ and glucose in the proximal convoluted tubule. SGLT2 inhibitors inhibit this transporter resulting in glycosuria, decreased serum glucose, and increased sodium delivery to the macula densa.

SGLT2 inhibitors may slow the progression of diabetic nephropathy by decreasing hyperfiltration and by decreasing the inflammatory and fibrotic response to hyperglycemia. This is supported by data from animal and in vivo models. Rats with DM treated with dapagliflozin show tubuloglomerular feedback activation and decreased glomerular filtration. In vitro studies show that empagliflozin attenuates the inflammatory and fibrotic effects of high glucose including expression of toll-like receptor-4, nuclear deoxyribonucleic acid binding to NF-κB and activator protein 1, collagen IV expression, and interleukin-6 secretion in human proximal tubule cells.
There are ongoing clinical trials to assess SGLT2 inhibitors’ ability to treat diabetic kidney disease as a primary outcome. Completed clinical trials with secondary renal outcomes show reason for excitement. The recently completed EMPA-REG OUTCOME trial compared empagliflozin to placebo in subjects with type 2 DM with a history of CVD and a eGFR≥30 ml/min/1.73 m2. Excitingly, this study found that treatment with empagliflozin reduced the risk of the primary composite outcome of death from cardiovascular causes, nonfatal myocardial infarctions, and nonfatal strokes! Analysis of prespecified secondary endpoints found that treatment with empagliflozin reduced the risk of progression to macroalbuminuria, risk of incident nephropathy, and doubling of serum creatinine.

Subjects treated with placebo showed steady decline in their eGFR throughout the study. Interestingly, there was an initial decrease in eGFR followed by stabilization of the eGFR in the empagliflozin group, reminiscent of what the RAS-i trials in diabetic nephropathy look like. Other SGLT2 inhibitors show renal-specific promise as well. The CANATA-SU trial compared canagliflozin vs glimepiride in type 2 DM and found a decrease in albuminuria in subjects treated with canagliflozin.
Though the early data is compelling, until the ongoing clinical trials assessing SGLT inhibitors ability to treat diabetic kidney disease as a primary outcome are complete, they have not yet been elevated to RAAS inhibition status. In the coming years, however, SGLT2 inhibitors may join the ranks of Gonzaga, Butler and Wichita State as yearly contenders in the Big Dance.
Glucagon-like Peptide 1 (GLP-1) Receptor Agonists

Copyright: Mehmet+Cetin / Shutterstock.com
GLP-1 receptor agonists preceded the SGLT2 inhibitors by a few years. Exenatide (Byetta) was introduced in 2005. GLP-1 is an incretin produced in the L-cells of the small intestine in response to ingestion of food. GLP-1 lowers glucose through its actions on the GLP-1 receptor by stimulating pancreatic beta-cells to secrete insulin, which in turn reduces plasma glucagon, slows gastric emptying, and suppresses appetite. The GLP-1 receptor has a wide distribution in the body and has been found in the pancreatic islets, central nervous system, lungs, gastrointestinal tract, heart, vasculature, liver, muscles, adipose tissue and in the kidneys.
| Exenatide | Byetta | 5-10 mcg SQ bid |
| Liraglutide | Victoza | 0.6-1.8 mg SQ daily |
| Lixisenatide | Available as Soliqua with insulin glargine and Adlyxin without | Once daily |
| Albiglutide | Tanzeum | 30-50 mg SQ once a week |
| Dulaglutide | Trulicity | 0.75 -1.5 mg SQ once a week |
| Semaglutide | Under investigation. Being developed as both an oral and injectable agent | |
The exact location of GLP-1 receptors in human kidneys is unclear. GLP-1 receptors have been found in rodent and porcine proximal tubular cells. In human kidneys they have only been found in hilar and intralobular arteries, but there is some methodological concern that currently available methods for detecting GLP-1 receptors are inaccurate. GLP-1 infused in obese men led to a significant increase in urinary sodium excretion, a decrease in proton excretion, and a decrease in the glomerular filtration rate suggesting an action at the level of the proximal tubule, perhaps at the level of the Na+/H+ exchanger. Rats with early type 1 diabetic nephropathy treated with the GLP-1 receptor exendin-4 had a decrease in albuminuria, glomerular hyperfiltration and a decrease in the release of pro-inflammatory cytokines. It is through these effects that GLP-1 agonists are hypothesized to have renoprotective effects in diabetic nephropathy.
While large scale clinical trials with primary renal outcomes are lacking, small studies and studies with secondary renal outcomes suggest that there are benefits. A small human trial of 23 subjects with overt diabetic nephropathy from type 2 DM were treated with liraglutide for 12 months which led to decreased proteinuria and a slower decline in eGFR. The LEADER trial is a large, recently completed study assessing cardiovascular outcomes in subjects with type 2 DM treated with liraglutide vs placebo. This was another exciting win for the cardiovascular team with a lower rate of the first occurrence of death from cardiovascular causes, myocardial infarction, or stroke in the group treated with liraglutide. Secondary renal outcomes from this trial were presented at ASN Kidney Week 2016. Subjects treated with liraglutide had a decreased risk of new onset macroalbuminuria, although time to persistent doubling of creatinine, ESRD, and death due to renal disease were similar in both groups.
While these agents have now been studied for over a decade demonstrating tremendous promise, they still have not crossed the goal line by showing a decrease in meaningful diabetic endpoints. GLP-1 receptor agonists are akin to Gonzaga, which has appeared in 19 tournaments and has been seeded 1, 2 or 3 five different times but has only made the Elite Eight once. With the team currently undefeated and ranked number one, could this be Gonzaga’s year?
SGLT-2 Inhibitors versus GLP-1 Receptor Agonists: How do they stack up?

– Post written and edited by Anna Burgner (@anna_burgner).
![]()
Leave a Reply