
Sustainable Kidney Care: Aligning Patient and Planetary Health
Mohamed Emlemdi is a medical student at The Ohio State University whose experience as a kidney transplant recipient has fueled his pursuit of a career in nephrology. He is passionate about organ donation awareness, transplant advocacy, and kidney research.
Amy Yau is an Assistant Professor of Clinical Medicine at The Ohio State University Wexner Medical Center Division of Nephrology with clinical interests in electrolytes and kidney stone disease. She participates in various FOAMed endeavors, such as the podcast “Channel Your Enthusiasm” and is passionate about patient and physician education.
Health care is responsible for a substantial share of national greenhouse gas emissions, rivaling that of major industrial sectors. Within medicine, dialysis stands out as one of the most resource-intensive therapies, requiring large volumes of water and energy, consumables such as single-use plastics, and waste from transportation. The environmental impact of kidney replacement therapies (KRT) is no longer a distant policy concern, but an emerging dimension of care that warrants closer attention.
In the January 2026 issue of AJKD, Saleem et al present a comparative lifecycle assessment of the environmental impacts of kidney transplantation, peritoneal dialysis, and hemodialysis. Using a standardized life cycle assessment (LCA) framework, they quantify greenhouse gas emissions and other environmental impacts including manufacturing of equipment and consumables, transportation, treatment delivery, and waste management. Their findings provide clear comparative data that distinguishes how different KRT modalities burden our environment. In-center hemodialysis had an approximately four-fold higher climate change impact than kidney transplant and about double that of peritoneal dialysis. Peritoneal dialysis showed the highest contribution to water depletion (41% of total impacts in that category) and metal depletion (~81%), reflecting the production and disposal of solutions and consumables.
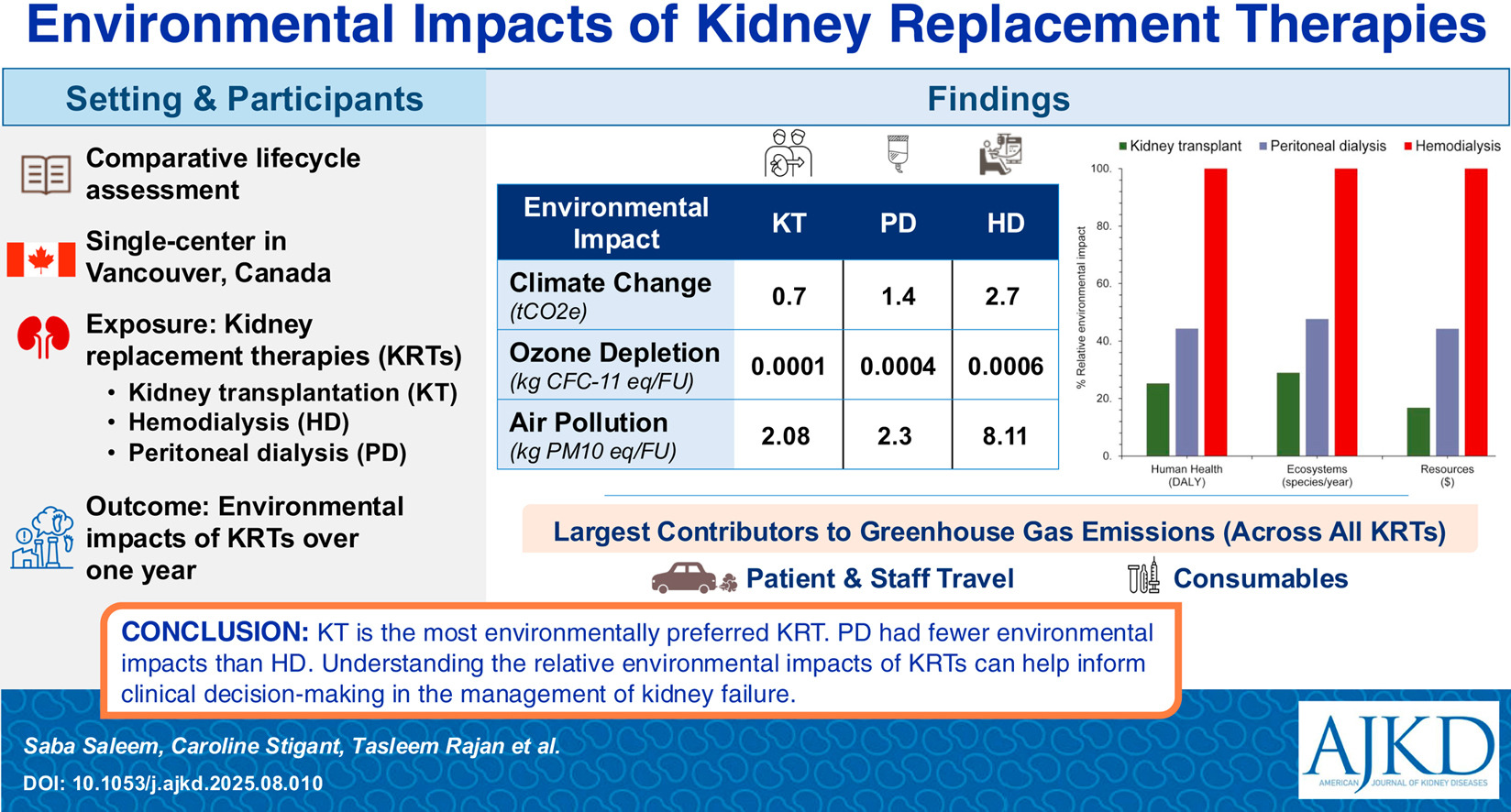
The central finding is striking but perhaps not surprising; kidney transplantation had the lowest overall environmental impact across nearly all assessed categories. Peritoneal dialysis generally demonstrated a smaller carbon footprint than hemodialysis, while in-center hemodialysis carried the greatest environmental burden. This was driven by frequent patient travel, high energy and water use, and single-use consumables including plastic circuits and dialyzers required during treatment sessions. In one LCA, for every 100 liters of water used in kidney transplantation, over 3,300 liters are consumed in hemodialysis, and more than 280 liters in peritoneal dialysis.
Comparable work on dialysis modalities has estimated annual per-patient emissions of approximately 4,800kg CO2e for in-center hemodialysis, about 3,000 kg CO2e for home hemodialysis, 3,300kg CO2e for automated peritoneal dialysis, and 2,000 kg CO2e for continuous ambulatory peritoneal dialysis. These results reinforce a consistent pattern: in-center hemodialysis is the most carbon-intensive option, home and peritoneal therapies have substantially lower emissions, and transplant generally has the lowest carbon footprint overall. Beyond greenhouse gases, dialysis exerts heavy pressure on water and natural resources, with in-center hemodialysis showing the highest overall environmental burdens across human health, ecosystems, and resource depletion indicators in the study’s comparative regional analyses.
These data invite a reframing of how the nephrology community approaches kidney care. As with any life cycle assessment, these results are context dependent. They reflect the local energy system, transport patterns, and clinical practices, so the main emphasis should be placed on the comparative patterns noted across modalities and not the exact values. On an individual level, for some patients, the idea that their treatment can be both life-preserving and less harmful to the planet may be a meaningful additional consideration. On a system-level, research should encourage timely referral for kidney transplant. One could view the low environmental impact of transplant relative to dialysis as a reflection of the superiority of kidney transplant, but also as an incentive to increase equitable access to transplantation. Of course, the environmental impact of KRT does not justify steering patients towards one modality or another; patients who cannot safely perform home therapies because of they lack the social support, resources, or reliable utilities may very well benefit from receiving in-center hemodialysis despite the higher environmental footprint.
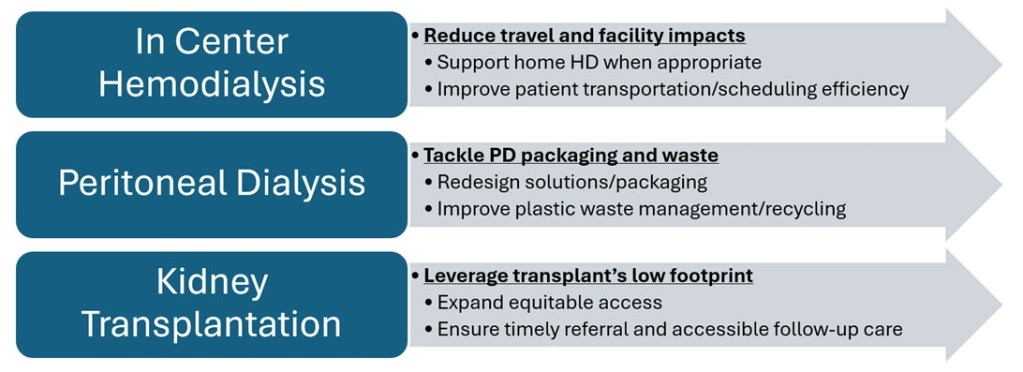
Figure 1: Clinical and system-level actions to lower the environmental impact kidney replacement therapies © Emlemdi and Yau.
The environmental impact of KRT also impacts how kidney services are designed and delivered. It can impact public policy and drive dialysis initiatives and innovations. In fact, the high water usage of dialysis has been well documented, and newer reverse osmosis (RO) machines may reduce reject water to as little as 10-15% compared to the 40% reject water rate by the study’s RO unit. This study helps identify concrete areas for decarbonizing kidney care. These lifestyle “hotspots” can be mapped to specific clinical and system-level actions (Figure 1). For instance, the predominance of travel-related emissions in hemodialysis suggests that expanding home hemodialysis programs and rethinking patient transport and scheduling could yield meaningful environmental gains without compromising care. For peritoneal dialysis, innovations in packaging, material choices, and waste management could address its high contributions to water and metal depletion.
The work by Saleem et al adds to our understanding of the environmental impact of KRT and helps us attain environmentally friendly kidney care. Achieving sustainable nephrology is likely to be built on small, concrete steps rather than a single transformative fix.
To view Saleem et al [Open Access], please visit AJKD.org:
Title: Environmental Impacts of Kidney Replacement Therapies: A Comparative Lifecycle Assessment
Authors: Saba Saleem, Caroline Stigant, Tasleem Rajan, Kasun Hewage, Rehan Sadiq, Andrea J. MacNeill, Christopher Nguan
DOI: 10.1053/j.ajkd.2025.08.010
Leave a Reply