
Lifetime Risk of CKD and the Implications for Screening
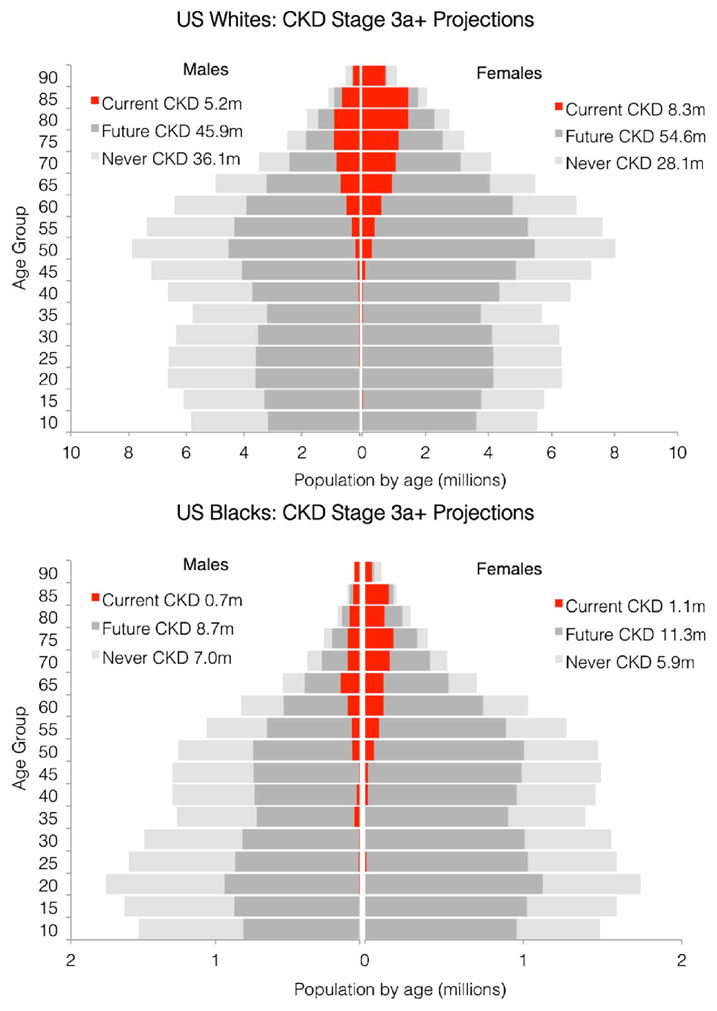
Fig 3 from Grams et al, © National Kidney Foundation.
Chronic kidney disease (CKD) is a common condition with multiple etiologies and important implications. The use of GFR estimation formulas is now ubiquitous in the medical field. The guidelines for CKD staging and management have greatly increased the awareness of this condition and highlighted its importance as a major public health problem. However, the true magnitude of the burden of CKD and the lifetime risk of this illness have not been previously well characterized. In the August issue of AJKD, Grams and colleagues use data from the National Health and Nutrition Examinations Survey to develop a Markov Model to estimate the lifetime risk of developing CKD based on estimated GFR and CKD staging guidelines.
The authors incorporate multiple data sources, including the National Vital Statistics Report, CKD prognosis consortium, and the US Renal Data System to construct a model that informs the overall lifetime risks of reaching individual stages of CKD (Stages 3a, 3b, and 4 as defined by the CKD EPI eGFR equation), and the ultimate risk of kidney failure or CKD stage 5. They estimate the probability of reaching each CKD stage and the probability of death prior to reaching ESRD for an individual of a baseline, age, sex, and race. These estimates are then complemented by more complex approaches that modeled CKD prevalence as a nonlinear function of age, and applying more conservative hazards for CKD associated mortality. Finally, they compare the findings of the Markov model to observed incidences from the Atherosclerosis Risk in Communities (ARIC) study, thereby validating the accuracy of their model.
The results from the model show that the average lifetime risk of acquiring CKD Stage 3A or greater is approximately 60% in the US population, and that it varies between 52% and 54% for black and white men, and 64% and 65% for black and white women. In comparison, the lifetime risk of developing ESRD is much higher in blacks, with risks for 8.5% for black men and 7.8% for black women, as compared to 3.3% and 2.2% for their white counterparts. These differential risks likely reflect a combination of genetic risk factors, disparities in health care, and differential rates of treated vs untreated early stages of kidney disease. Risk estimates for Hispanics and other high risk ethnic groups could not be estimated due to lack of data from NHANES.
These findings highlight the important public health burden of CKD, and provide appropriate comparison with other chronic conditions that have a similar lifetime risk. The risk of developing CKD (approximately 60%) was higher than the lifetime risk of diabetes (33-39%), but lower than the risk of hypertension (approximately 83%). Indeed, as the accompanying editorial by Kiberd points out, you can now add CKD to the familiar Benjamin Franklin adage that “the only certain things in life were death and taxes.”
However, this study is not without limitations, and these should be pointed out. First, Hispanics are not addressed in this study as NHANES data are not sufficient to examine this population. Secondly, this study only examines risk of each stage compared to normal kidney function, and not progression through sequential stages. This is an important point and one that warrants further investigation. What are the risk factors that explain if a person transitions from stage 3 to 4 to ESRD?
Although kidney failure requiring renal replacement therapy remains uncommon, the recognition of CKD as a common disease should lead to more aggressive screening efforts in high risk groups, such as younger blacks, and certain at-risk elderly populations. In this regard, the early identification of CKD may potentially lead to early and appropriate treatment of hypertension, management of cardiovascular risk factors, and a reduction in acute kidney injury episodes through prevention of safety hazards. On the public health front, the high estimates of lifetime risk should help raise awareness in the community and push health policy makers and funders to back efforts to understand and treat kidney disease. The study by Grams et al should provide further evidence that CKD is indeed a common, harmful, and a treatable problem.
Navdeep Tangri, MD, PhD, FRCPC
Assistant Professor, Division of Nephrology, University of Manitoba
eAJKD Contributor
To view the article (freely available), please visit AJKD.org.
Leave a Reply