
#NephMadness 2018: Contrast Region
Submit your picks! | NephMadness 2018 | #NephMadness | #ContrastRegion

Copyright: Lightspring / Shutterstock
Selection Committee Member for the Contrast Region:
Paul M. Palevsky, MD
Dr. Palevsky is a Professor of Medicine in the Renal-Electrolyte Division at the University of Pittsburgh and Chief of the Renal Section at the VA Pittsburgh Healthcare System. Dr. Palevsky is a clinical researcher who has helped lead a number of landmark studies in the treatment of AKI and CKD. Follow him @PaulPalevsky.
Competitors for the Contrast Region
Contrast is Nephrotoxic vs Contrast is NOT Nephrotoxic
Gadolinium in CKD4 vs Iodinated Contrast in CKD4
Contrast is Nephrotoxic vs Contrast is NOT Nephrotoxic
Acute kidney injury (AKI) has been known to occur after iodinated contrast administration for over 6 decades. Previously (and still) called contrast-induced nephropathy (CIN), the nomenclature changed to contrast-induced acute kidney injury (CI-AKI) and now contrast-associated acute kidney injury (CA-AKI). What explains this shift in nomenclature? It is our understanding about the true nature of AKI after contrast that has changed over time. Safer contrast agents, better patient selection, and greater awareness of the inherent confounding has resulted in the questioning of the existence of this entity itself. Let’s unpack the layers of this causation versus association conflict in our scouting report for the Contrast Region.
Contrast is Nephrotoxic

Copyright: keantian / Shutterstock
Raise your hand if you have seen a patient with AKI due to contrast administration (and if you didn’t raise your hand, either you are not a nephrologist, or, ahem, you need to brush up on your diagnostic acumen!). So why are people proclaiming that contrast induced AKI (CI-AKI) is a myth? Or that the most common cause of hospital-acquired AKI does not exist? Should a bunch of retrospective ‘big data’ dredging studies and a meta-analysis count more than what you seen with your own eyes? Can the big data wish away the patient you dialysed the other night with pulmonary edema, a mere 2 days after their coronary stent? Let’s unpack the literature to understand where this confusion about the evanescent CI-AKI stems from.
The original CI-AKI case report dates back to Bartels and colleagues’ description of AKI after intravenous pyelography in 1954 (cited in this report a few years later). Over the subsequent decades, there has been extensive research into the pathophysiology, prevention, and treatment of CI-AKI. The diagnosis of CI-AKI is based on an acute rise in serum creatinine (Scr) over 24 to 72 hours following administration of contrast media, and exclusion of other causes for AKI such as atheroemboli, among others. Despite older studies reporting a risk of CI-AKI as high as 20%, more recent studies have reported an incidence of 0.8-1.7%. On the basis of the former numbers, dating from a study over 3 decades old, contrast is often cited as the 3rd most common cause for AKI in the hospital. That is no longer true, and we will be right with you protesting against that hyperbole. But it still exists, as we shall see.
The osmolality of contrast agents played a huge role in the high incidence of AKI in the early years, when the osmolality of the contrast agents used (eg, diatrizoate) ranged from 1,500 to 2,000 mOsm/kg. About 2 decades ago, on the basis of a meta-analysis of 31 trials, it was conclusively shown that low osmolar contrast agents are safer (pooled OR, 0.61). Since then, there has been a complete shift to using low-osmolar agents (low here means lower than high-osmolar agents, but not lower than plasma osmolality), with osmolarity ranging from 550 to 700 mOsm/kg. The data on low versus iso-osmolar agents is less definitive, with ORs ranging from 0.46 to 0.97 (lots of heterogeneity in meta-analyses depending on specific agents and route of administration). Along with the consideration of cost, this explains why the usage of iodixanol, the prototypical (and only one on the market) iso-osmolar contrast agent, has not swept the field like the low-osmolar agents did a few decades ago.
What other factors have led to a decreased risk of CI-AKI? We use lower doses of contrast, and improved technologies have opened the door to to more non-contrast imaging and magnetic resonance imaging. Risk scores allow physicians to risk stratify patients in order to avoid contrast in the most risky patients.

Another factor in the changing perception of CI-AKI is its soft definition: previously a 25% rise in Scr at 48 to 72 hours, though now the AKIN and KDIGO criteria are used. Small rises of Scr are quite common in sick patients—who are also more likely to have contrast procedures—and the contrast procedure is a convenient smoking gun. Little attention has been paid to the last part of the CI-AKI definition—the absence of other etiologies, and hence CI-AKI has been truly overcalled.
However, the recent flurry of database papers suggesting CI-AKI does not exist are similarly bombastic and on shaky ground. They take patients who have not received contrast and compared them to similar patients who did receive contrast. The similarity is presumed on the basis of sophisticated statistical techniques—you will find words like ‘propensity score matching,’ ‘marginal structural modelling,’ and ‘machine learning algorithms’ thrown in their methodologies.
But when you have 2 very similar patients: why is a clinician going to decide not to give contrast to one but give contrast to the other? Because using their clinical gestalt that a patient is at higher risk of AKI, they withhold contrast! This selection bias cannot be adjusted away by statistics, and is at the root of the machine oversimplifying human decision making.
Then there is this study, the biggest of the big data studies, with almost 8 million hospitalizations. What it purports to show is that not only is contrast not associated with higher risk of AKI, but that contrast is associated with lower risk of AKI. Before you start talking of the renoprotective effects of contrast, consider that the big data wasn’t big enough to tell you if contrast was given before or after the AKI. Surely you can see the reverse causation here, apart from the same selection bias we discussed before?
People have foolishly called the AMACING trial as the last nail in the coffin for CI-AKI. Really? All it showed was that intravenous (IV) fluid expansion does not prevent a soft definition of AKI from happening in low to intermediate risk patients. Like Mark Twain, one has to conclude that the reports of the death of CI-AKI have been greatly exaggerated.
If that doesn’t satisfy you, recent studies have documented that AKI continues to occur with contrast procedures in prospective controlled settings, especially in high-risk individuals. In a study comparing the incidence of AKI in those who underwent iodinated contrast imaging vs those who underwent imaging with carbon dioxide, the incidence of AKI was higher in contrast group (4% [CO2 group] vs. 11% [contrast group]; OR, 0.465).
If you like database and statistics, well, a propensity-matched study showed that patients with Scr ≥ 1.6 mg/dL had a significantly higher risk of CI-AKI when compared to controls who underwent unenhanced imaging studies. And if someone tells you this is as good as it gets, there is an ongoing randomised trial, of iodixanol versus placebo in 1,164 patients with advanced CKD, which we are confident will show that contrast does cause AKI. We call it for #KidneyWk2021.
In conclusion, IV or intra-arterial contrast is still nephrotoxic in high risk individuals—i.e. those with underlying advanced chronic kidney disease (CKD) or with other reasons for renal hypoperfusion, and especially when they receive high-dose contrast. Avoid giving contrast in such patients if you can, and use adequate precautions such as low- or iso-osmolar contrast, low contrast volume, and volume repletion if you can’t. Call the nephrologist if the patient does develop oliguria 24-48 hours after the contrast. Maybe then you will believe in the existence of contrast-induced AKI.

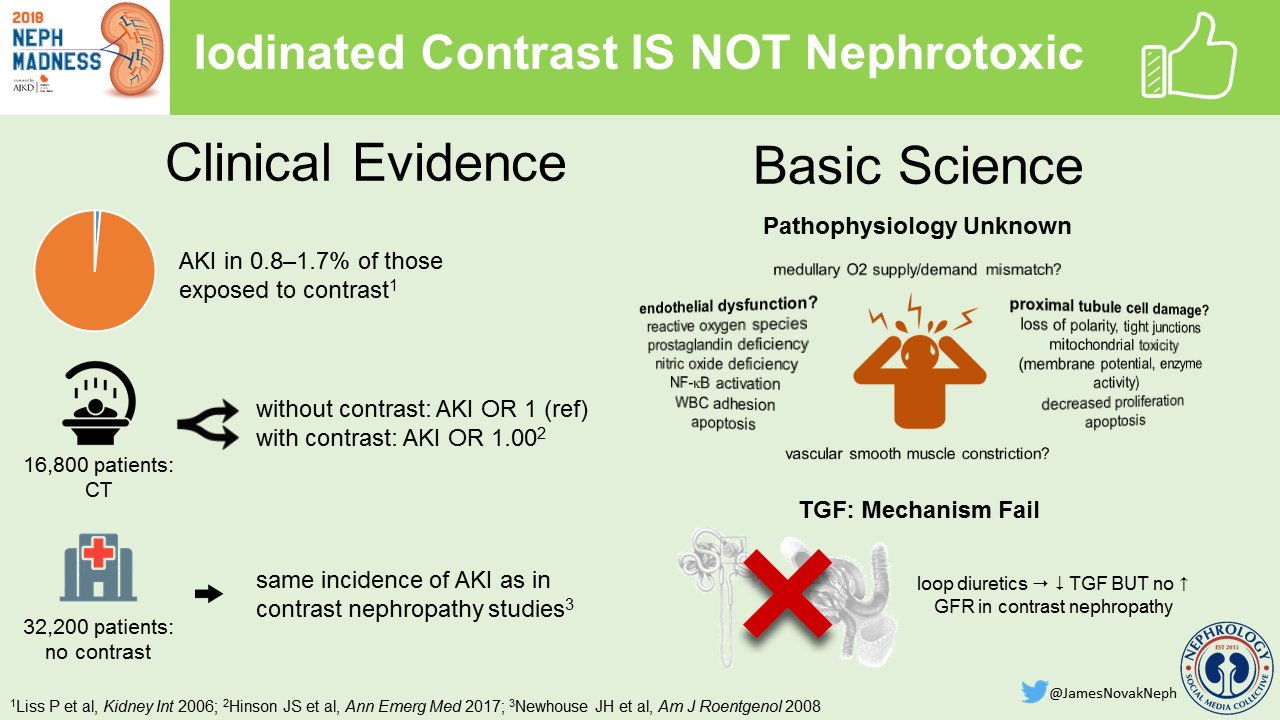
Contrast is NOT Nephrotoxic

Copyright: Mike Pellinni / Shutterstock
CI-AKI legitimately has an existential crisis today. The temporal relationship of contrast administration to the rise in Scr is easy to detect in a patient in the hospital where daily chemistry panels are routinely performed. However, association does not establish causation. AKI after contrast is not necessarily due to the contrast. We repeat, association is not causation. To call AKI in a patient with vascular disease, sepsis, underlying CKD, who, by the way, has had a recent contrast-enhanced computed tomography (CT) scan, as contrast-induced is just plain lazy! Hence there has been a move afoot to replace CI-AKI to contrast associated AKI (CA-AKI), or even post-contrast AKI.

But with so many associations, surely there is fire beneath the smoke? If one wants to establish causation, we need to have a good animal model, not complicated made-up flowcharts. There is not a convincing animal model, unlike in hypertension or cisplatin-induced AKI. It doesn’t help that the precise mechanism of AKI has never been completely elucidated and most flow charts attempting to explain the mechanism of kidney injury from contrast look like a complex maze of words and bi-directional arrows. Adenosine, endothelin, prostaglandins, reactive oxygen species, hypoxia, and physical properties of the contrast such as viscosity and osmolarity are just some of the purported hypothetical pathophysiological mechanisms. All of which suggests confusion rather than clarity.

Wong et al, Int J Cardiol.
So let’s look towards human studies instead. Randomized trials where some patients receive contrast, and others don’t, are a bit challenging to perform, that one could only dream about. Large databases, which contain a lot of data about contrast procedures as well as patient demographics, comorbidities, and treatment details can help tease out the role of contrast. The first shots were fired in this study of 32,000 hospitalised patients, none of whom had received contrast. Over half of them had a 25% rise in Scr, and more than 40% would have fulfilled the AKIN criteria. Without receiving contrast. If the background rate of AKI is so high in hospitalized patients, should one correctly call CI-AKI instead as ‘hospital-acquired AKI’? Despite the tongue-in-cheek element of that statement, this does reveal how often such AKI can easily blamed on an incidental contrast study, where contrast is merely an innocent blameless bystander.
And there is better-quality data. In a large, retrospective, propensity score-matched analysis from the Mayo Clinic, the incidence of AKI was similar between patients who received CT scans with IV contrast and those who underwent unenhanced CT scans. In the same issue of the journal, the group also published a meta-analysis of 13 retrospective studies which compared AKI in patients undergoing CT scans with IV contrast to other imaging studies without IV contrast and concluded that incidence of AKI were similar between the 2 groups. More recently, another large study of patients seen in the emergency department, using logistic regression and propensity score matching, reported a perfect OR of 1.00 for risk of AKI with contrast versus controls, as defined by the KDIGO criteria.
The last aspect is the soft definition of CI-AKI, based on changes in Scr—which are so common in hospitalized patients. Since kidney biopsies are uncommonly performed in this setting, we can look towards biomarkers of kidney injury—surely if contrast is causing medullary hypoxia and acute tubular necrosis, there should be evidence of this? This was somewhat supported by a study looking at two AKI biomarkers (NGAL and KIM-1) in which urinary excretion of these 2 biomarkers were similar in the group that developed CI-AKI and in the one that did not develop AKI. The authors conclude that there is no evidence of any tubular injury in patients who have AKI after contrast. Contrast is like Keyser Söze, the devil we have been programmed to fear, which doesn’t even exist.
Why should it matter though, beyond academic interest, whether contrast does or does not cause AKI? Is CI-AKI or CA-AKI just a matter of squabbling semantics? Consider that the risk of CI-AKI is considered highest in patients with underlying CKD. Also consider that these patients are in general sicker, have more coronary disease, and are more likely to be hospitalized for various reasons. But they are denied necessary coronary angiograms, angiographic procedures, contrast-enhanced CT scans in fear of causing CI-AKI. This exacerbates the therapeutic nihilism in CKD patients, aptly titled ‘renalism.’ The nephrology community needs to stamp out this madness (truly NephMadness) of CI-AKI and do appropriate imaging as needed for all our patients.
Gadolinium in CKD4 vs Iodinated Contrast in CKD4
When it comes to patients with advanced CKD, imaging studies rapidly become very tricky. Giving them iodinated contrast for enhancing studies, and they may develop AKI and end up quickly on dialysis. For years magnetic resonance imaging (MRI) with gadolinium was thought to be the safer alternative but we now know it may cause the deadly nephrogenic systemic fibrosis (NSF). What should we do—is one of these options safer, or more accurately, which option is less unsafe?
Gadolinium in CKD4
Gadolinium (Gd), named after its discovery in the 19th century in the mineral gadolinite, is the commonest contrast agent used in MR imaging. Although free gadolinium is quite toxic (and lethal to animals at 100 mg/kg), the chelated molecule is way less so. Its paramagnetic property makes it very attractive to allow blood vessels and tissues to illuminate with MR imaging. And it is not nephrotoxic, so prior to 2006, Gd-based contrast agents (GBCA) were commonly used instead of iodinated contrast in patients with CKD in order to avoid the dreaded CI-AKI. But an Austrian nephrologist and the FDA changed all that in 2006, by linking a fatal systemic fibrosing condition to GBCAs.
Gd and Nephrogenic Systemic Fibrosis
The story begins in 2000, when Shawn Cowper, a dermatologist from Yale, reported a peculiar skin condition which resembled scleroderma, with thickening of the skin and collagen remodelling on skin biopsies. All 15 patients with this skin condition, which he labelled ‘nephrogenic fibrosing dermopathy,’ were on dialysis and the skin condition was thought to be yet another complication of kidney failure. Over the next few years, it was seen that this fibrosis was not restricted to the skin—it was systemic and in particular, it occured in the pleura and diaphragm, causing respiratory failure. The disease, now named nephrogenic systemic fibrosis (NSF), was slowly progressive, but eventually fatal.
As Cowper’s registry increased with cases being reported worldwide, the only factors seemed to include being on dialysis (for ESKD or AKI), having vascular disease, getting IV iron, and metabolic acidemia. It took 6 more years before an observant Tom Grobner made the link with Gd: five of his dialysis patients showed skin changes within 2-4 weeks of MR angiography, and he bravely speculated that Gd was to blame. On a quick review, Gd was detected within stored tissue samples (despite up to 11 months’ delay from MR and skin biopsy), Gd was found to cause fibrocyte differentiation in vitro, and almost all cases in the NSF registry were found to have prior Gd exposure.
The dominant GBCA at that time was gadodiamide (Omniscan) and it wasn’t initially clear whether it was Gd, or this particular agent which was to blame. As it turns out, it was most likely a combination. The major factor to keep in mind is the really long lag period—though Grobner noted it in weeks, the skin changes may manifest years after the Gd exposure. This likely led to the 6-year delay in making the link, but also suggests there may be patients walking around who will manifest NSF in the coming years. Lastly, there is a dose-response relationship, with a greater risk associated with higher volume of Gd and with multiple doses of Gd.
Risk Factors: The Gadolinium-Based Contrast Agent
Gadolinium is chelated to a carrier molecule that reduces the toxic effects of a free Gd ion. The theory of Gd causing NSF requires the Gd to become free of this Gd-chelate complex, a process called ‘transmetalation.’ Naturally, the type of chelate bound to each gadolinium affects how tightly Gd is bound, with higher affinity binding leading to lower amounts of Gd release. Properties such as ionicity, structure (linear versus macrocyclic), and thermodynamic stability are some physicochemical attributes thought to associate with this propensity and subsequent NSF risk. Based on the actual reported risk, the American College of Radiology (ACR) has classified the Gd compounds into groups as shown in the table.

The ACR Classification of GBCAs with respect to NSF risk, modified from the ACR manual
Names in parentheses refer to brand names; confounded = cases where two different Gd agents were associated.
Again, given the lag period, take this grouping as tentative—Omniscan was the first and widely used MR agent, which is why most NSF cases have been reported after the same. Newer agents have not been around for a long enough period of time—and additionally we have become much more careful with Gd exposure in patients on dialysis, so this often represents lack of evidence of harm rather than evidence of absence of harm.
Risk Factors: Kidney Function
GD is a necessary factor when it comes to NSF, but is clearly not sufficient, given the vast numbers of Gd-MR imaging studies happening daily and the small and dwindling number of cases of NSF now being reported. The other risk factor is poor kidney function, with most cases being on dialysis. Why would NSF be more likely to occur in patients on dialysis? Several factors, the most important of which is a markedly prolonged half-life of the chelate in circulation, thus a greater opportunity for transmetalation, with the additional factor being the metabolic milieu of uremia contributing. Most of the cases have indeed been reported in patients on dialysis, the vast majority in patients with ESKD. A few cases have been reported in patients with AKI, with patients with AKI not on dialysis having a milder form, and with resolution of NSF symptoms if renal recovery occurred.
In patients who are already on dialysis, one should weigh the risks and benefits of NSF, and if Gd is indeed necessary, the ACR recommends dialysis immediately after, though the European guidelines suggest there is no role for dialysis. Indeed, dialysis does remove Gd efficiently, but cases of NSF have been reported despite dialysis after administration. Moreover, the metabolic milieu will be most favorable for transmetalation in the hour before dialysis, arguing that the Europeans do have a point. In addition, there is no evidence that immediate or more intensive dialysis mitigates the risk of NSF. How about patients with advanced CKD and who are not on dialysis? Should one start them on dialysis? Should one not use Gd-MR imaging at all in those patients, and if so, where does one draw the line?

Copyright: VILevi / Shutterstock
MR Imaging in Advanced CKD
MR imaging does have certain advantages and is mandatory for accurate imaging of the certain areas, such as the nervous system and the hepatobiliary system. To relegate a patient with advanced CKD who has neurological or liver disease to non-Gd imaging is therapeutic nihilism padded with the precautionary principle. The risk of NSF with eGFR < 30, and not yet on dialysis is not zero, but pretty close. The few cases reported were with the use of group I agents (see table above), and no cases have been reported of NSF with group II agents and non-dialysis-dependent (NDD) CKD. One could argue that if MR imaging with non-Gd contrast agents are available, one could use those instead, e.g. ferumoxytol, or non-enhanced MR imaging using spin phase effects or time-of-flight sequencing, though they will not always be available or suitable for your clinical needs.
What about doing a contrast-enhanced CT scan, using iodinated agents instead? Even the most avowed obituarist of CA-AKI will still accept that there is a risk of AKI after contrast when the eGFR is already so low. A small rise of 25%-50% in Scr may be all you need to push the CKD stage 4 patient over the edge. The resultant oliguria and fluid overload will quite often necessitate starting dialysis. Immediately. Weigh that against the very small (likely <<<1%) lifetime, long-term risk of NSF with the lower risk group II agents. The choice will light up brighter than any contrast agent.
In conclusion, to quote the European guidelines, “An unfortunate result of anxieties about NSF has been that enhancement during MRI may be avoided inappropriately and important disease overlooked. In a patient with mild or moderate renal impairment, the risk of NSF from an MR examination enhanced with one of the most stable gadolinium-based agents is likely to be less than the risk of nephrotoxicity from a CT examination enhanced with an iodine-based agent.”
Iodinated CTA for CKD4

Copyright: Suttha Burawonk / Shutterstock
Iodinated contrast has been around for a long, long time. Estimates of contrast use, from 2003, were 80 million doses, corresponding to 8 million liters of iodinated contrast in humanity. If you are a strong believer in contrast causing kidney failure, this volume of contrast could explain the entire CKD epidemic! Having read the scouting reports above, however, we know that the risk of contrast causing AKI is very low overall with judicious use of modern low- or iso-osmolar agents. Paradoxically, among patients still considered to be at some risk of AKI, namely those with CKD 4 or 5NDD, the need for contrast enhanced procedures is very high. Perhaps they need it for vein mapping prior to access creation, or after access creation they have an underdeveloped arteriovenous fistula and need an angioplasty.
Advanced CKD also associates with accelerated atherosclerosis. The treatment for the ensuing unstable angina and acute coronary syndrome almost always includes iodinated contrast injected into the coronaries. Patients with CKD also have the other usual indications for angiograms and CT scans: cerebrovascular and peripheral vascular disease, cancer, and so on. What should one do? Treat CKD patients as second-class citizens, forever condemned to renalism? You might have opted for gadolinium-enhanced MR imaging in a naive era a decade or so ago, but the deadly scourge of nephrogenic systemic fibrosis has annihilated Gd use in CKD. Let us boldly make the case for using contrast in advanced CKD.
True Contrast AKI almost always recovers
The fear of iodinated contrast, and the hurdles with ‘renal clearance,’ aka approval of the nephrology service before a contrast imaging test is done in a CKD patient, mainly stem from the fact that it is very much an iatrogenic insult, rather than the magnitude of the renal tubular injury involved. The natural history of contrast-induced AKI is that of a rise within 24 to 48 hours, peak Scr value by 3-5 days, and resolution to baseline in the next few days. This is very much unlike true acute tubular injury, backed by the lack of data showing a rise in biomarkers such as NGAL or KIM-1. Indeed, if your patient with presumed contrast-induced AKI has not recovered within 2 weeks, an alternative diagnosis such as atheroembolic renal disease or acute tubular necrosis should be strongly considered. So your patient with CKD stage 4 has a Scr bump after a contrast test? No need to fuss, just tighten the seat belt and ride that rise back down to baseline.
Existing prophylactic measures are extremely efficacious
Given that AKI after contrast was first reported in 1954, and we know when we are administering this potentially nephrotoxic agent, a cornucopia of prophylactic agents have been trialled to protect the kidney. Solomon first described the benefit of volume expansion, with a seminal trial which reported 0.45% saline alone being superior to saline + mannitol or furosemide. A few years later, the idea of using 0.45% saline alone being the best approach quickly fell by the wayside to 0.9% saline instead. The subsequent saline wars have been unbalanced, however, with Merten’s description of the superiority of a bicarbonate-based fluid taking over a decade to be reversed, despite some valiant attempts.
Another salient saline scenario is to give larger amounts, using left ventricular end-diastolic pressure to guide you, or with matching diuresis with furosemide. Both these strategies are resource intensive, and have not been widely reproduced after the initial trial. Perhaps oral salt and water could be simpler and cheaper? However, very few events from very few trials are available, to say anything conclusively. How about statins, which prevent everything from coronary artery disease to cancer? If we are considering adding them to drinking water, why not before a contrast imaging test? There is some evidence to support that, and even if you doubt its robustness, it is hard to argue against the sharp logic of using statins in this population. Low- and iso-osmolar agents, discussed above, already lower the risk of AKI significantly, and are exclusively used in this era.
The last and most controversial measure has been the smelly, sulfurous N-acetyl cysteine (NAC). First described in 2000 by Tepel to dramatically decrease AKI in patients with CKD undergoing contrast-enhanced CT scans, there was never any proper mechanistic explanation for its efficacy. Subsequent studies varied greatly in showing or not showing its purported beneficial properties. An excellent meta-analysis and a large trial, albeit in lower risk patients, failed to sway NAC believers. It took a Veterans Affairs-funded trial to finally reverse this, by testing NAC vs placebo, as well as bicarb vs saline in a 2×2 factorial design. In one fell swoop, PRESERVE showed the lack of superiority of both these strategies.
Lastly, with modern imaging technology, a very small amount of contrast (< 30 mL) is sufficient for angiography and and stenting, with zero AKI reported in 30 patients with advanced CKD. So saline (or bicarb, if you are fixated on it), using a small amount of low- or iso-osmolar contrast results in a minimal risk of AKI after contrast.
To conclude, whether you believe or disbelieve the concept of contrast-induced or contrast-associated AKI, adequate prophylactic measures should not preclude using iodinated contrast even in patients with GFR < 30. Get your patient with CKD4 the angiography they need and the stent they deserve.
– Post prepared by Swapnil Hiremath (@hswapnil), Anitha Vijayan (@VijayanMD), Natasha Dave (@NatashaNDave), and Rajeev Raghavan (@jeevsmd).
How to Claim CME
US-based physicians can earn 1.0 CME credit for reading this region. Please register/log in at the NKF PERC portal. Click on “Continue,” click on the “Contrast Region,” then click on “Continue” to access the evaluation. You’ll need to click on “Continue” again to complete the evaluation, after which you can claim 1.0 credit and print your certificate. The CME activity will expire on June 15th, 2018.
Submit your picks! | NephMadness 2018 | #NephMadness | #ContrastRegion
I agree completely that nephrologist should not be put in a position to answer the question is a contrast study suitable when the referring physician and radiologist cannot decide. The referring physician is overall in charge and should make the call and the radiologist should only advise but not forward the issue to a third part such as the nephrologist.
Great analysis
Thanks