
#PathPointer: Membranous Nephropathy in the Era of Mass Spectrometry
PathPointers highlight important everyday teaching points when reviewing kidney histology. These brief and easy-to-read blog posts include real clinical images to demonstrate various biopsy findings.
A 75-year-old man with a history of diabetes, hypertension, osteoarthritis, and NSAID use developed nephrotic syndrome characterized by anasarca and a urine protein:creatinine ratio of 11.5 g/g. His serum creatinine was 1.23 mg/dL; ANA, ANCA, complement C3, C4, SPEP, UPEP, serum free light chains, hepatitis B, C, HIV were all negative/normal. He was up-to-date on cancer screening and had no history of malignancy.
Kidney biopsy demonstrated membranous nephropathy (MN) superimposed upon histologically mild diabetic glomerulopathy with mild mesangial sclerosis without nodularity on light microscopy. MN was characterized by faint subepithelial “spikes” and “holes” in the glomerular basement membrane. These “spikes” represent the reaction of the glomerular basement membrane to the subepithelial immune deposits while the immune deposits appear as negative space or “holes” on Jones stain, or in red on trichrome stain. Immunofluorescence showed glomerular granular capillary wall staining for IgG, with codominant staining for IgG1 and IgG3, and a lesser degree of staining for IgG4 and IgG2. PLA2R was negative. Electron microscopy revealed widespread deposition of subepithelial immune deposits without features suggestive of secondary membranous nephropathy (no subendothelial or mesangial immune deposits).
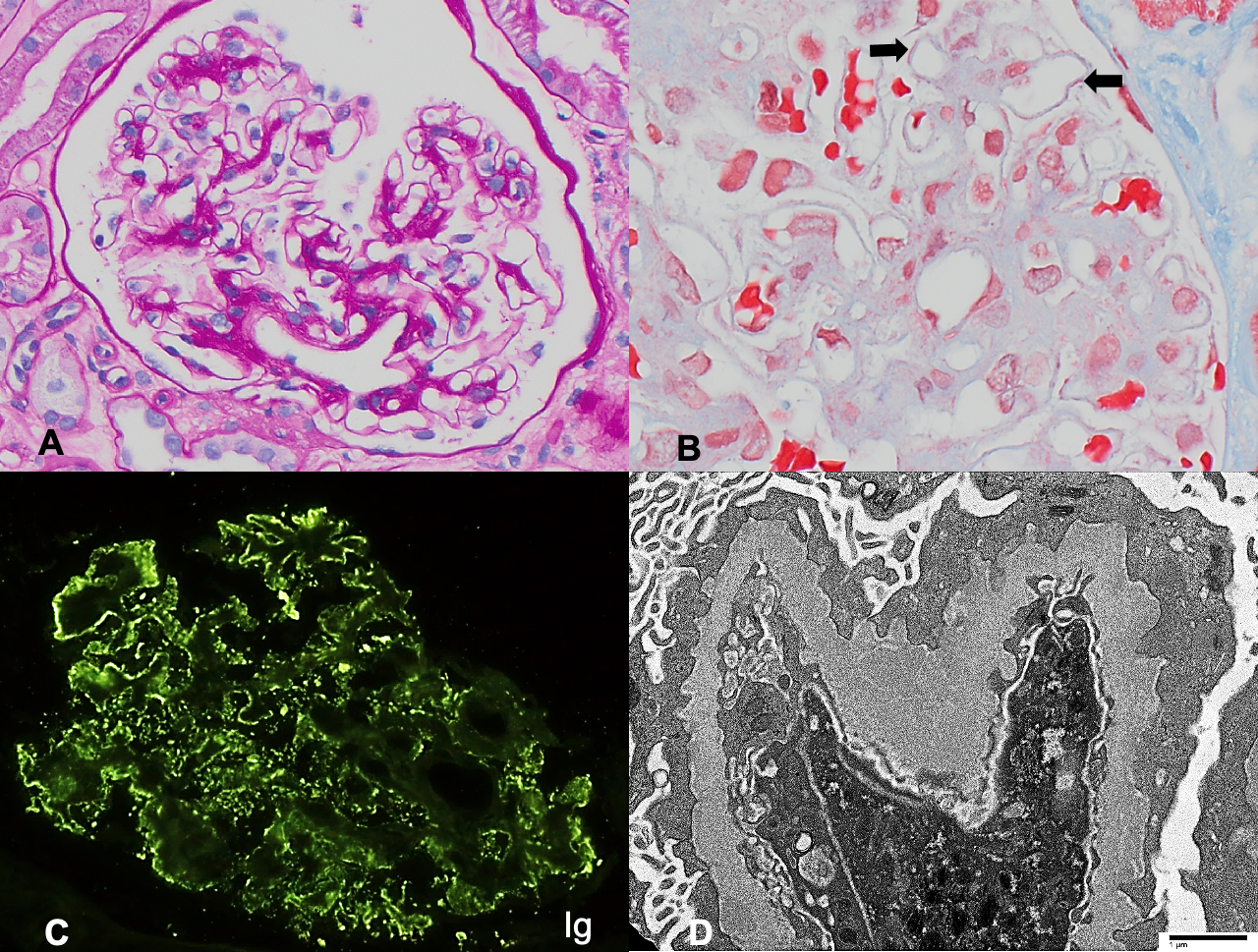
A. Mild mesangial expansion on PAS stain, consistent with underlying diabetic glomerulopathy (200x). B. Subepithelial immune deposits characteristic of membranous nephropathy appear red on trichrome stain (arrows, 600x). C. Immunofluorescence demonstrates granular peripheral capillary wall staining for IgG. D. Electron microscopy shows subepithelial immune deposits and diffuse podocyte foot process effacement, without subendothelial or mesangial deposits (direct magnification 4800x).
Approximately 80% of MN are “primary,” or kidney-limited, and 20% are “secondary,” or associated with systemic diseases (autoimmune, infectious) or exposures (gold, mercury). About 70% of primary MN are due to autoantibodies to phospholipase A2 receptor (PLA2R), a podocyte antigen. Anti-PLA2R–negative MN raises the possibility of a secondary MN, prompting evaluation for systemic disease. However, recent serologic and mass spectrometry studies have rapidly expanded our knowledge of other podocyte antigens involved in apparently primary or secondary MN.
Specifically, antibodies to thrombospondin type I domain-containing 7A (THSD7A) are seen in 3% of patients with MN, or 10% of anti-PLA2R–seronegative patients. Similar to PLA2R, anti-THSD7A antibodies are usually of IgG4 subclass. Rare cases of primary MN are dual-positive for PLA2R and THSD7A within immune complex deposits on immunofluorescence of the kidney biopsy. The THSD7A antigen shares some biochemical features with PLA2R, and its epitope was shown to have high sequence similarities with PLA2R dominant epitopes, suggesting that this shared motif may be a common pathway to developing MN.
In contrast to PLA2R-associated MN, however, THSD7A-associated MN is more commonly associated with neoplasia. Malignancy has been reported in approximately 20% of cases of THSD7A-positive MN, with overexpression of THSD7A demonstrated in the tumor and lymph node metastases in some cases, providing a potential paraneoplastic mechanism for development of MN. Thus, evaluation for an occult malignancy should be considered in cases of anti-THSD7A–positive MN.
In addition to the THSD7A antigen, investigators utilizing mass spectrometry and immunohistochemistry have identified specific overexpression of exostosin 1 and 2 (EXT1/EXT2) in secondary MN associated with autoimmune disease. Most of these patients were young women and had laboratory findings suggesting an underlying autoimmune disease (positive ANA, dsDNA, SSA/SSB, RNP antibodies); nearly half had a clinical diagnosis of lupus or mixed connective tissue disease. Concordant with the clinical scenario, renal biopsy findings clearly suggested secondary MN in 85% of these cases, demonstrating “full house” staining for C1q, IgA, IgM, and/or IgG1 dominant immune deposits by immunofluorescence, and/or subendothelial or mesangial immune deposits or endothelial tubuloreticular inclusions by electron microscopy.
Finally, neural epidermal growth factor-like 1 protein (NELL-1) is a recently discovered autoantigen in anti-PLA2R–negative MN. Most reported NELL-1–associated MN cases are seen in older adults without systemic conditions or underlying malignancy, although a few have had cancer. Initial studies suggest that NELL-1–associated MN represents 16% of anti-PLA2R-negative primary MN. On renal biopsy, NELL-1–associated MN lacks the typical features of secondary MN (described above), but may be IgG1-dominant, in contrast to anti-PLA2R and anti-THSD7A–associated MN. Given the lack of systemic conditions in the described patient above, he may represent a case of anti-NELL-1–associated primary membranous nephropathy.
Taken together with clinical and renal biopsy findings, recent serologic and mass spectrometry studies are quickly advancing our understanding of other antigens involved in development of anti-PLA2R–negative membranous nephropathy. In a patient with anti-PLA2R-negative MN and no evidence of systemic disease or malignancy, identification of antibodies to THSD7A or NELL-1 in the kidney biopsy may provide biologic insight, a more precise diagnosis, and eventually may lead to targeted treatment.
– Post prepared by Nicole Andeen, AJKDBlog Contributor
Leave a Reply