
Impact of Moral Distress on Nephrology Providers
A recent Policy Forum offers an international perspective on moral distress in nephrology in diverse contexts and health care systems. AJKD Social Media Editor Timothy Yau @Maximal_Change (AJKDBlog) interviewed one of the authors, Samantha Gelfand @SammyG (SG), about how this issue contributes to personal and professional dissatisfaction, and steps that need to be taken to foster resilience.
AJKDBlog: In this article, you begin by defining moral distress, which “occurs when individuals are unable to act according to their ethical beliefs due to external factors.” Moral distress leads to frustration, burnout, and if extreme or prolonged, may cause one to abandon the field. Do you have a personal example of how you have experienced this during your medical training?
SG: My most serious experience of moral distress occurred in my role as a nephrology fellow. It’s tough to offer a single example because unfortunately it was an iterative experience. As inpatient consultants, we navigate multiple juxtaposed worlds in the course of a day, from the emergency department to surgical intensive care units to transplant services. The level of agency for a consultant (let alone a fellow!) in each of these settings is highly variable, and it took a long time for me to develop a language to express the frustration and disenfranchisement I sometimes felt in that role. There were times when I felt that we were asked to dialyze patients without being allowed to engage fully in what I consider to be ethical care, which includes a careful review of risks, benefits, prognostic meaning, and patient-centeredness of the intervention. I found a good deal of support and community in my co-fellows and attendings, though I think we can do more to discuss and address moral distress in clinical training programs.
AJKDBlog: I think your awareness of this during fellowship training is really important to acknowledge, and makes it imperative that we have strategies to counter the frustration. Another really important point highlighted in this Policy Forum is that moral distress is not something that only healthcare providers face – patients and family members experience moral distress as well. We’ve all encountered difficult end-of-life discussions or decisions that clash due to a belief system. Why do you think the patient experience of moral distress has received such limited attention in medical literature?
SG: This is a fascinating reflection. I agree that this is not a common topic in the literature, and yet some of the most famous cases of patients’ or surrogate-decision makers’ moral distress are Supreme Court cases! Why isn’t it a focus of medical literature? To start, in the history of academic medicine, the patient experience is a relatively new area of interest, and the qualitative tools needed to study it are not always as well understood or definitive as classical quantitative methodologies purport to be.
Second, I think it’s a reflection of the power dynamic that underlies the patient-clinician relationship: in much of modern medicine, medical expertise and “standard of care” trump the cultural and spiritual belief systems that contribute to an individual’s sense of what is right or ethical. This becomes apparent in the vocabulary we use to describe these situations, “clashes” or “conflicts” or even “ethical dilemmas,” terms which technically refer to a situation where multiple ethical principles are in conflict with each other (versus considering that a patient or family member might be experiencing actual moral distress, where the ethical path appears clear to them but unattainable). I think it is a fascinating area for further study in nephrology, where patient experience and decisional regret are likely to be highly related to patient outcomes, provider satisfaction, and it must be said, cost.

Table 1 from Ducharlet et al, AJKD © National Kidney Foundation
AJKDBlog: This is something that we are all experiencing, whether we are aware of it or not. There is probably no “one-size fits all” solution, but what are the steps we need to think about to alleviate moral distress at the individual level?
SG: The first step is to name it. Sometimes language is a precursor to awareness. We should use the term “moral distress” on a regular basis. It can transform the vague experience of “being upset or frustrated” into a defined and actionable entity. Otherwise, feelings that go unnamed and unexamined evolve into other more familiar things such as anger, resentment, impotence, hopelessness, and worst, detachment.
AJKDBlog: Last question, and this one’s harder for me to answer based on the paper. As medical education is changing, it’s important that learners from all levels (undergrad, med school, residency, fellow, and beyond) have the right tools to deal with moral distress. Often, learning these skills is referred to as the “hidden curriculum.” How do we bring this knowledge and these skills out of the shadows and into formal learning?
SG: Now more than ever, I think educational leaders are starting to solicit input and elevate voices from learners who used to be considered low on the hierarchy of speakership. Social media platforms like Twitter have helped with this. The COVID-19 pandemic, unfortunately, may have helped too, given the unprecedented clinician moral distress on a national level, which has led to a national dialogue about vulnerability, disempowerment, and mental health. My hope is that these topics remain explicit and become ingrained in medical education.
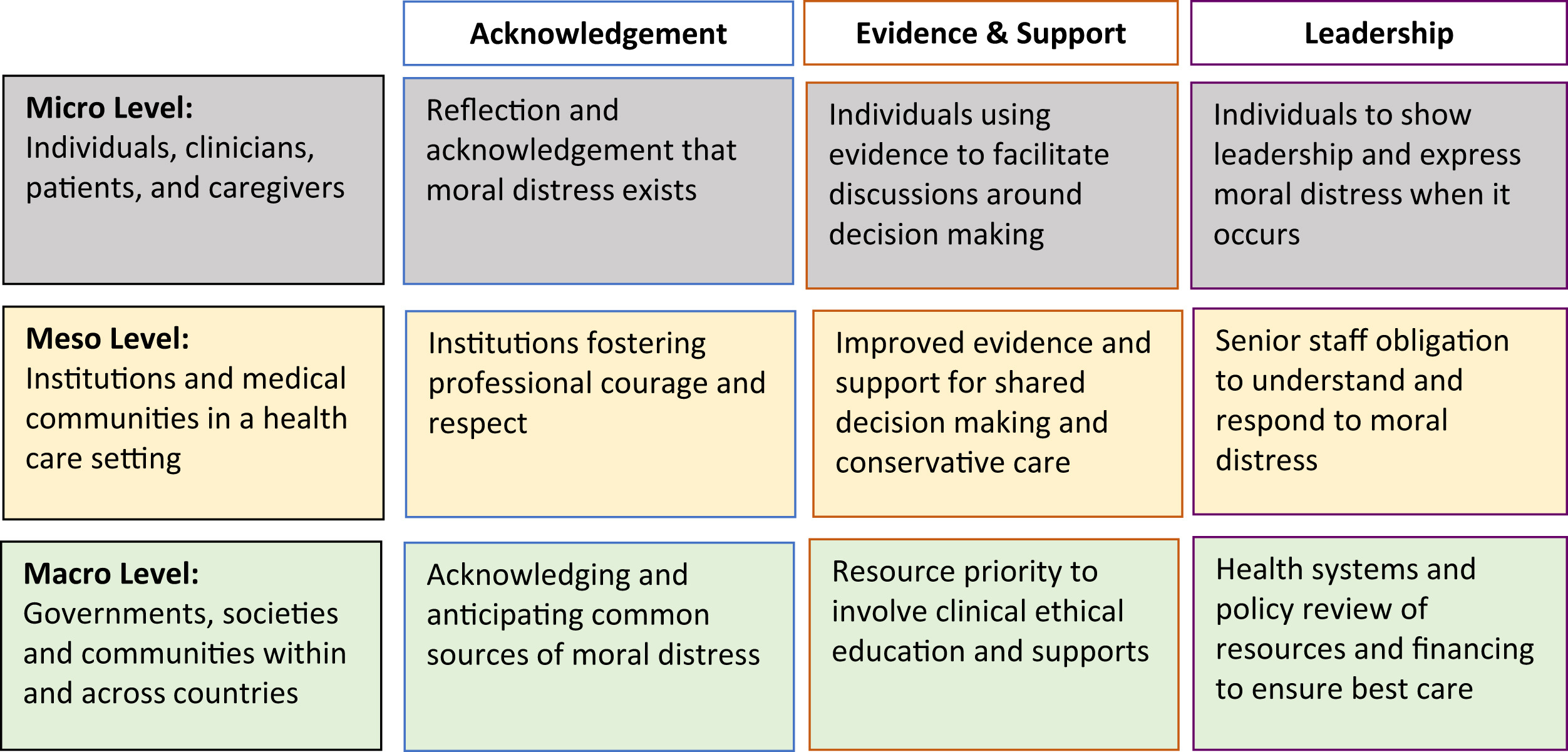
Strategies for addressing moral distress in nephrology. Figure 1 from Ducharlet et al, AJKD © National Kidney Foundation
How do we see to this? In my view, an explicit moral distress curriculum would start with modeling. Leaders and seasoned clinicians need to discuss their own experiences of moral distress with each other, in front of trainees. This is so much harder than it sounds – it requires a top-down willingness to be vulnerable, which is not easy! And yet it can be done with thoughtful implementation. Most training programs already have structured curricula involving case reviews, whereby cases are usually presented by the trainee (student, intern, resident, fellow) and commented upon by more experienced practitioners. Case conferences tend to focus on challenges in diagnosis and management of disease. In my experience, reflecting on ethical dilemmas or emotionally challenging cases tends to be relegated to a separate venue, either “reflection rounds” or Schwartz Rounds. It’s an asset to have such venues, but it also may act as a disservice, a form of “othering” for this kind of discussion, as though it is not as central to clinical practice as medical facts and assessments.
One way to formalize our approach to discussing moral distress is to include it within our discussions of diagnosis and management of disease. It would require some bravery, including using the words “I” and “we” more often than customary in our current shibboleth. It would require release from the Oslerian ideal of equanimity, a willingness to acknowledge and examine and share our own reactions to the complex situations in which we work. I am hopeful that regular discussion will validate the topic and hopefully dispel some of anger, frustration, and shame that can lead to clinician injury.

Box 1 from Ducharlet et al, AJKD © National Kidney Foundation
To view the Ducharlet Policy Forum (FREE temporarily), please visit AJKD.org.
Title: Moral Distress in Nephrology: Perceived Barriers to Ethical Clinical Care
Authors: K. Ducharlet, J. Philip, H. Gock, M. Brown, S.L. Gelfand, E.A. Josland, and F. Brennan
DOI: 10.1053/j.ajkd.2019.09.01
Leave a Reply