
A Decade of Progress: Reducing Cardiovascular Morbidity in Chronic Kidney Disease
Bertram Pitt is professor emeritus of the University of Michigan School of Medicine where he spent 15 years as the director of the Division of Cardiology. His research in practically all areas of cardiovascular disease includes special emphasis on ischemic heart disease and heart failure. Dr. Pitt is the author of almost 500 papers and chapters in books and has served on the editorial board on a number of journals in cardiovascular disease.
Michael Holinstat is a Professor of Pharmacology at the University of Michigan who studies platelet biology, hemostasis, and thrombosis. Dr. Holinstat holds numerous patents on novel therapeutic drugs developed to prevent or treat rare thrombotic diseases. Additionally, Dr. Holinstat has published more than 130 peer-reviewed articles in the area of regulation of blood flow, hemostasis, thrombosis, and platelets function.

Chronic kidney disease (CKD) is associated with a number of major adverse cardiovascular events (MACE) including an increased risk of arterial and venous thromboembolic and bleeding events. As such, it is imperative to determine which interventions or therapeutic regimens are having the greatest positive impact on patients with CKD and whether these interventions are reducing morbidity and mortality outcomes in this patient population. In order to assess whether approaches to treatment over time have impacted patient outcomes, it is necessary to be able to evaluate all patients in a given region and follow their treatment. Utilization of national registries is likely one of the best mechanisms for capturing this information over time across a large population.
In a recent issue of AJKD, Faucon et al. used the Nationwide Swedish Registry to evaluate trends in the rates of thrombosis and bleeding from 2011 through 2021. The authors found that the absolute burden of cardiovascular and bleeding events increases progressively with CKD severity with the highest incidence rates observed among patients on peritoneal dialysis for cardiovascular endpoints and among hemodialysis patients for bleeding. Second, when compared to an age- and sex-matched general population, the relative excess of risk is striking: the standardized incidence rate ratio (IRR) for MACE ranged from approximately 2-fold in CKD G4 to >3-fold in peritoneal dialysis, and the standardized IRR for major and non-major bleeding events ranged from ~5-11-fold across CKD stages and dialysis modalities. These data reaffirm that advanced CKD carries a cardiovascular hazard that exceeds what would be expected based solely on age and comorbidities.

Their trend assessment demonstrated that while the morbidity and mortality outcomes of patients with CKD have continued to increase compared to the population, reductions were observed in MACE as well as arterial and venous thromboembolism. Interestingly, while major bleeding events decreased, clinically relevant non-major bleeding increased. This is of high interest, and it will be important in the future to determine the underlying reasons for the inverse relationship between major and non-major bleeding in this cohort.
The decreased MACE and thromboembolic events may be due to the decrease in the use of antiplatelets, increased use of anticoagulants, and uptake of SGLT2 therapy and lipid-lowering medications in these patients. The development and use of sodium glucose transporter-2 (SGLT2) inhibitors have increased as the co-morbidity of diabetes in this patient cohort continues to rise. SGLT2 inhibitors have shown a positive effect in heart failure which may explain their contributing role to decreased MACE risks in patients using SGLT2 inhibitors as part of their therapeutic regimen.
While these outcomes are promising, our understanding of therapeutic intervention in CVD, especially as it pertains to CKD and diabetes, may enable even further reduction in morbidity and mortality in these patients. In the area of SGLT inhibitors, for example, we now recognize that some SGLT inhibitors such as the dual SGLT1 and SGLT2 inhibitor sotagliflozin likely affects blood coagulation and clotting in addition to its beneficial effects on glucose control and cardiac protection. Further, the study noted that while newer interventions like SGLT2 inhibitors have shown a positive outcome for CKD patients, RASi use was very limited. Increased RASi, nonsteroidal mineralocorticoid receptor antagonists, GLP1-RA, and combination therapy including novel antiplatelet or anticoagulant therapy in this population may result in an even further decrease in MACE in this population.
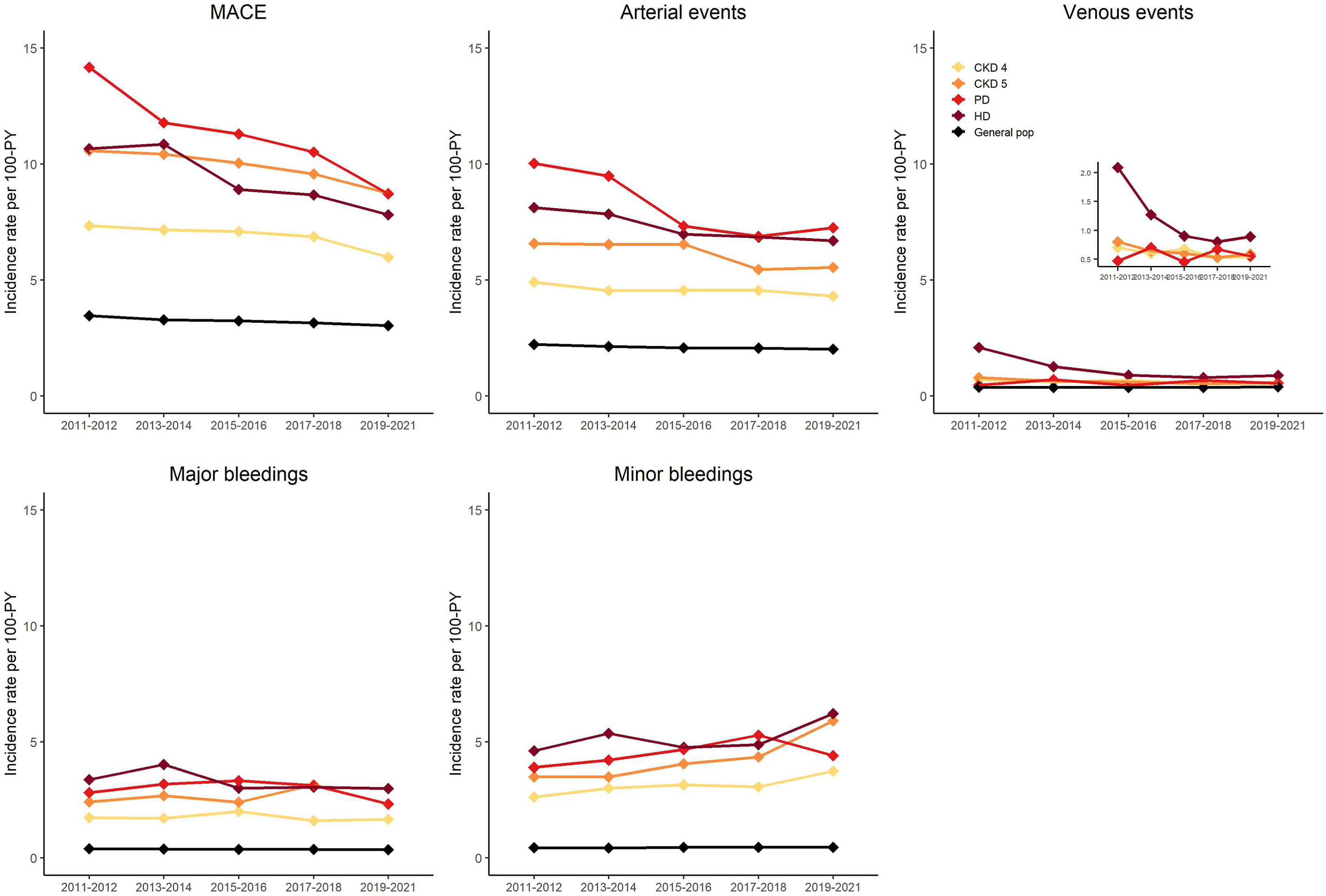
Temporal trends in the incidence rates of study outcomes in patients with advanced CKD and in the general population. In each cohort and for each 2-year calendar block, event rates were calculated per 100 PY. MACE (major adverse cardiovascular events) is defined as cardiovascular death or hospitalization for myocardial infarction or stoke. Arterial events are defined as hospitalization for myocardial infarction, ischemic or undefined stroke or transient ischemic attack, acute lower limb ischemia, or systemic arterial thrombosis/embolism. Venous events include deep vein thrombosis, pulmonary embolism, and systemic venous thrombosis. “Minor bleeding” refers to clinically relevant non-major bleeding events. Figure 1 from Faucon et al, © National Kidney Foundation.
Limitations to the Swedish retrospective cohort is that this represents only one country and its treating guidelines. Evaluating other country-wide registries may uncover a different set of benefits based on their treatment guidelines. The study also lacks granular data on indications, dosing, and adherence.
Future meta-analyses including these registries are necessary to gain a larger picture of how interventions in patients with CKD have changed over time and how these changes are impacting outcomes. Future meta-country analyses may also uncover differences in age, sex, and co-morbidity differences unique to specific geographic regions. Overall, while CKD co-morbidities and mortality continue to be a significant burden on society, the major associated pathology of MACE, arterial and venous thromboembolic events, and bleeding have decreased over the past decade due in large part to the use of a variety of therapeutic approaches. Continued implementation of guideline-directed therapy and the development of new agents may lead to an even lower morbidity and mortality in these patients and the information attained can be used to evaluate if these interventional approaches may be expanded to other regions of the world.
To view Faucon et al [Subscription required], please visit AJKD.org:
Title: Trends in Major Cardiovascular Events and Bleeding Among Patients With Advanced CKD: A Nationwide Swedish Study
Authors: Anne-Laure Faucon, Stefania Lando, Shunsuke Murata, Morgan E. Grams, Edouard L. Fu, Frida Welander, Nazleen F. Khan, G. Brandon Atkins, Irina Barash, Dena R. Ramey, Karin Modig, Marie Evans, Juan-Jesús Carrero
DOI: 10.1053/j.ajkd.2025.08.011
Leave a Reply