
NephMadness: The Final Four!
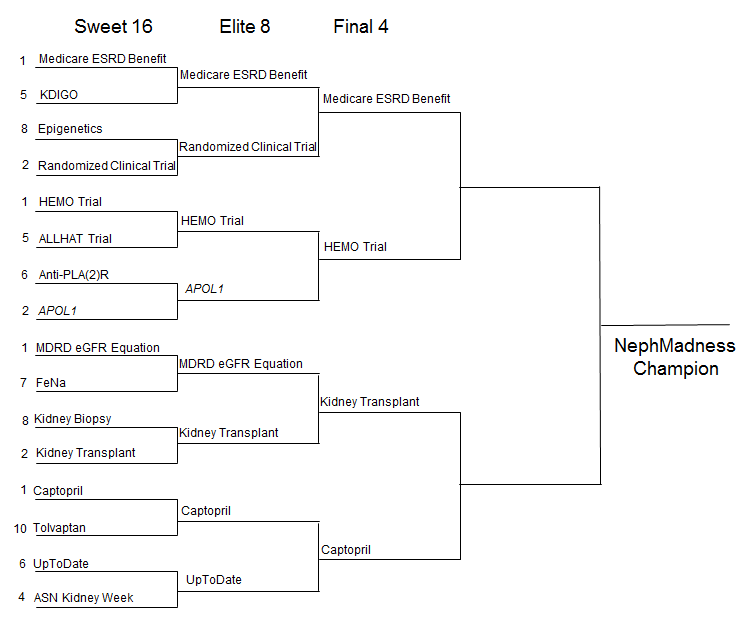 The people have spoken. The votes have been tallied. And now we have the honor to present the first NephMadness Final Four:
The people have spoken. The votes have been tallied. And now we have the honor to present the first NephMadness Final Four:
-
Medicare ESRD benefit
-
HEMO trial
-
Captopril
-
Kidney Transplantation
Each one changed the landscape of nephrology in a unique way. We are going to tally the votes for the final 4 voting period between April 2- April 8 and award the NephMadness championship to the achievement with the highest cumulative votes. Click here for updated brackets. Let’s look at the contenders for Nephrology Madness Champion below:
(1) Captopril
Captopril is a heavy favorite to win the NephMadness championship.
Captopril has already taken down the transplant drug mycophenolate and now has to take on the entire transplant enterprise (this could be a daunting task). Captopril is a heavy hitter and has spawned the creation of several classes of drugs. Each of which inhibits either the production or action of angiotensin II. Most notably are the angiotensin converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARBs) and the direct renin inhibitors. In a sense Capropril is the grand daddy of them all. These drugs are ubiquitous to nephrology and have shown positive results in several clinical trials, a true UCLA of the field. The first reports of Captopril (AKA SQ 14,225 or D-2-methyl-3-mercaptopropanoly-L-proline) came in 1977 in Lancet in which 14 volunteers received the oral drug and showed promise in decreasing blood pressure. The history of how the ACEis were discovered is discussed in more detail here. Captopril really turned on the afterburners in 1993 when Ed Lewis, as part of the collaborative study group, dropped the results of the Captopril vs. Placebo randomized controlled trial in insulin-dependent diabetes:
Captopril treatment was associated with a 50 percent reduction in the risk of the combined end-points of death, dialysis, and transplantation that was independent of the small disparity in blood pressure between the groups
Two months earlier the results of the Diabetes Control and Complications Trial (DCCT) research group published how intensive insulin treatment to lower glucose delays the onset and slows the progression of diabetic retinopathy, nephropathy, and neuropathy in patients with type 1 diabetes. Effectively, laying the groundwork for how diabetes is still being treated today. Arguably, these few months in 1993 may be the most important in the history of internal medicine literature.
(2) Kidney Transplant
Lets look at Kidney Transplant. As noted by Pascale Lane in her NephMadness blog post, Kidney Transplant remains the closest thing we have to a cure for kidney disease right now. And, as far as solid organ transplants go, is a very viable option for a wide variety of patients with ESRD. According to the NIDDK about 18,000 kidney transplants are performed in US every year. However, about 90,000 patients are on the waitlist. In short, there aren’t enough kidneys to go around. We have come a long way in terms of immunosuppression, surgery, post-op care, living donor surgery and tissue typing that have all culminated in reduced graft failure since the first transplants were performed. However, over the last 10 years these trends have stabilized. Well, lets take a look at diabetes and ESRD.
The estimated survival of a patient with diabetes on dialysis is only 30-40% at 5 yrs, while kidney transplantation increases their 5 yr survival to up to 70% for a cadaver kidney transplant, and to up to 80% for a living donor kidney.
It’s hard not to vote for kidney transplant. Wow.
(1) Medicare ESRD benefit
Medicare ESRD benefit has been rolling over the competition, burying in order: Transplant chains, PD First, and KDIGO. It wasn’t until it came up against the randomized controlled trial that there was a bump in the road. It was close with, RCT taking the Medicare benefit to overtime in a nail biter, but the entitlement won out earning a birth in the first NephMadness Final Four.
The randomized controlled trial is the life force behind the advancement of medical science. The RCT is the closest we can get to pure truth in our desire to unlock the secrets of the human body, but this is nephrology, a specialty that, to its discredit, has blundered forward with only a smattering of RCTs. So perhaps it is fitting that Treasure trumped Truth.
And what a treasure it is, it could be argued that the field of nephrology has as much to thank Richard Nixon, who signed the act, as Homer Smith. The ranks of nephrology has swelled as our patient population grew. In 1972, when the act was signed, there were 10,000 Americans with ESRD. Today that number approaches half a million. Dialysis units dot the landscape of inner cities, rural towns and suburban strip malls. This is an achievement that has truly changed Nephrology, our patients and America itself.
(1) HEMO Trial
The final contender is the HEMO trial. Another landmark in the world of dialysis and one that should quell any euphoria over Medicare’s ESRD benefit’s defeat of the RCT in the Elite Eight. HEMO overturned twenty years of growing observational data pointing to significant benefits from increased low molecular weight molecule clearance. This shocked the nephrology world and shows the value of well done definitive RCTs. It also shows the tremendous value that can come from a negative trial.
One of my favorite memories of HEMO: we were discussing the trial with the fellows and one of them asked what HEMO stood for. This was because every study name has to be based on an acronym, no matter how much of a hack it is. I wrote John Daugirdas and he sent me a note saying, “nope HEMO is just hemo, short for hemodialysis.”
So simple, so honest.
Leave a Reply