
The Yin and Yang of Autophagy in Kidney Ischemia Reperfusion Injury
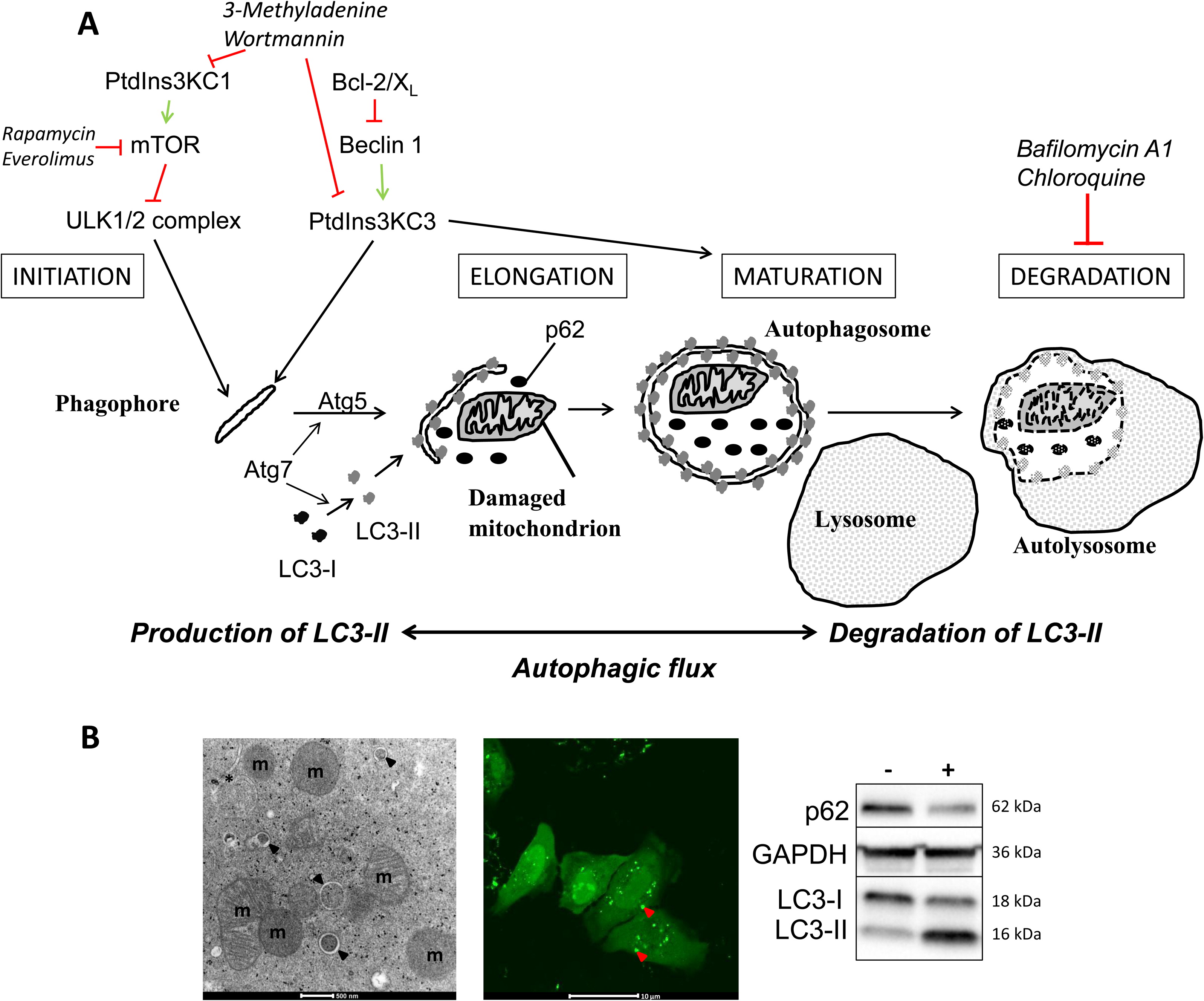
Overview of autophagy and the common monitoring techniques. Fig 2 from Decuypere et al AJKD, © National Kidney Foundation.
The components that make up a cell are in constant flux. New proteins are made and old ones are degraded. What happens to these partially degraded or damaged intracellular constituents (proteins, organelles) as a cell ages? If these damaged proteins were to accumulate, they could jeopardize cellular function and lead to improper function. Therefore, a process termed autophagy (Greek “auto” meaning self and “phagos” meaning eat) exists to help clean up this cellular debris by shunting it to lysosomes for degradation. We are just beginning to unravel this complex process as it relates to many diseases processes. A recent article by Decuypere et al in AJKD explores the role of autophagy in kidney ischemia-reperfusion injury and therapy. The authors provide an overview on where we are in potentially exploiting this therapy for novel treatments of acute kidney injury (AKI).
It is clear that the process of autophagy is a complex process, intertwined in other important cellular fate determinates such as apoptosis. From a general concept once would think enhanced autophagy would be a good thing. If you have an injured cell, turning on a system responsible to clearing out damaged cellular debris should help the cell survive. But how do you turn on or off the autophagocytic system and measure response?
This can be done by a variety of means, such as overexpressing key autophagy proteins such as Bcl-2 or knocking out autophagy protein 5 or 7 (Atg5,7) and assessing how AKI is affected. Treatment with drugs known to affect autophagy, such as everolimus, tacrolimus, MMF, furosemide, resveratrol, or bafilomycin A1 (for example), can also be applied. Interestingly, results from approximately 15 animal studies in which autophagy was altered (Table 1) yielded mixed results. Some models demonstrated beneficial effects while others showed detrimental effects in experimental AKI (ischemia reperfusion injury (IRI)). This is a technique where one or two renal arteries are ligated for a period of time (30 min to 1 hour), and then released causing AKI. Why such a varied response? The authors speculate that the duration of ischemia really matters. If the ischemic event is limited to 25-40 minutes, autophagy is protective. In contrast, if the event is prolonged to 40-60 minutes, autophagy is detrimental and leads to autophagy-dependent cell death. What is also curious is that gender might also alter the response. They hypothesize a dual role of autophagy to explain the sweet spot of autophagy to be protective (Figure 4).
Can this system be modulated for therapeutic benefit? The interesting point is that many commonly used drugs affect autophagy, and if deployed correctly could decrease the degree of AKI from ischemic insults, such as during cardiac bypass surgery or kidney transplantation. What is also interesting to speculate is whether we are already altering autophagy (a key cellular process) with the use of immunosuppressive drugs like everolimus, tacrolimus, MMF, and even the common diuretic furosemide. What we are lacking is a magic bullet to modulate the system with precision without causing adverse effects. Much more research is needed before we can begin to imagine a potential therapy. The review by Decuypere et al demonstrates how it will be necessary to carefully dissect these pathways in animal models before attempting to translate these findings to humans.
Dr. Matt Sparks
AJKD Blog Advisory Board member
To view the article abstract or full-text (subscription required), please visit AJKD.org.
Leave a Reply