
In-Center Nocturnal Dialysis: What Do We Know?

Photo: Pixabay / metsi
There has been mounting evidence that home nocturnal hemodialysis (conducted 5-6 nights/week) has various benefits compared to conventional thrice-weekly in-center hemodialysis (HD). These benefits include decreased blood pressure, improved indices of mineral metabolism, decreased medication use, and improved quality of life. However, the use of home nocturnal dialysis can be limited by factors such as poor social support, lack of personal resources, comorbid conditions, and fear of self-cannulation. For these patients, in-center nocturnal HD (conducted 3 nights/week with each session lasting up to 8 hours) could be an option.
In a recent publication in AJKD, Wong et al conducted a systematic review of the literature to determine the effects of in-center nocturnal HD versus conventional HD on various clinical outcomes. These outcomes include blood pressure control, left ventricular hypertrophy, markers of anemia and bone mineral metabolism, nutrition, quality of life, sleep quality, frequency of intradialytic hypotension, hospitalization, and mortality.
After extensive review of the literature, 21 articles met the selection criteria and were included in the analysis. All studies were observational and a total of 1,165 patients were treated with in-center nocturnal HD vs 15,865 patients treated with conventional. The breakdown in various outcomes is listed below:
Blood pressure: 15 of the included studies reported blood pressure parameters; of these, 6 showed improvements of these parameters (mainly systolic blood pressure [SBP]) with in-center nocturnal dialysis and 4 showed a concurrent reduction in the use of antihypertensive medication. Pooling of date showed a mean SBP difference of -2.45 [95% CI, -4.12 to -0.78] with no difference in diastolic blood pressure (DBP) between groups.
Left Ventricular Hypertrophy: 5 studies measured left ventricular hypertrophy; 4 of these studies showed a statistically significant reduction in left ventricular mass in patients undergoing in-center nocturnal HD.
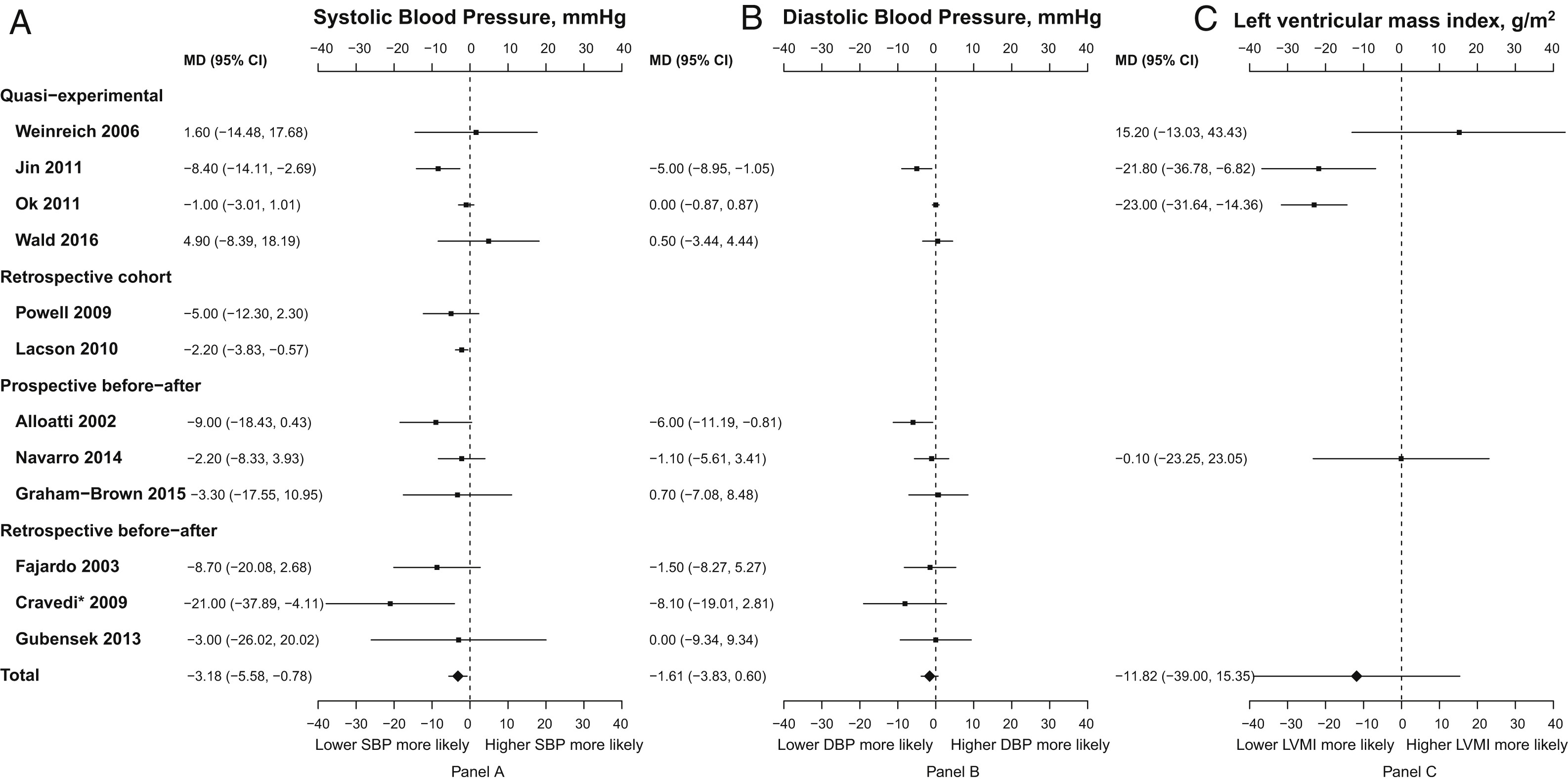
Forest plots for blood pressure and left ventricular hypertrophy outcomes. (A) Predialysis systolic blood pressure (SBP), (B) predialysis diastolic blood pressure (DBP), and (C) left ventricular mass index (LVMI). ∗In sensitivity analyses for predialysis SBP, Cravedi 2009 was excluded; mean difference (MD), −2.45 (95% confidence interval [CI], −4.12 to −0.78) mm Hg. For each panel, estimates on the left side of the axis show that participants in the in-center nocturnal hemodialysis group are more likely to have lower SBP (or DBP or LVMI), while estimates on the right side of the axis show that participants in the in-center nocturnal hemodialysis group are more likely to have higher SBP (or DBP or LVMI). Figure 2 from Wong et al, AJKD © National Kidney Foundation.
Bone Mineral Metabolism: 15 studies included measures of bone mineral metabolism. 11 studies revealed a reduction in predialysis phosphate in patients undergoing in-center nocturnal HD, with a reduction in use of phosphate binders seen in 2 of these studies. Pooled data show a mean reduction in serum phosphate by 0.97 mg/dL [95% CI, 0.46 to 1.48]. Effects on PTH and calcium levels were too confounded to result in a clear signal for change.
Other: Outcomes for hospitalization, mortality, nutrition, sleep, and quality of life were reported in a supplemental document. The sample size was small for the detection of meaningful difference, but no outcome was worse in the in-center nocturnal HD treated group.
Despite Wong et al being the first in-depth review of clinical outcomes in in-center nocturnal HD, there are several limitations that need to be noted. Significant inconsistency in reporting outcomes among the studies make pooling of outcomes difficult. Moreover, the use of observational and quasi-experimental studies (which dominate this literature in the absence of RCTs) has its own set of limitations. Finally, the majority of studies had fewer than 40 participants, making statistically significant conclusions difficult to make. Although difficult to answer, one final consideration is that patients who choose 5x/week nocturnal dialysis may be more compliant than standard in-center dialysis patients when it comes to issues such as phosphate binder, fluid, and diet adherence.
In conclusion, although it is difficult to make practice recommendations based on this review, it was noted that in-center nocturnal HD was associated with improvement in SBP, hemoglobin concentration, and serum phosphate levels. Similar conclusions have been made in other trials looking at more frequent dialysis treatments (eg the FHN trial), which imply that time may be the most important variable in KT/V. Larger, well-designed clinical trials are needed to provide certainty about the true risks, benefits, and cost-effectiveness of in-center nocturnal HD.
– Post prepared by Abdo Asmar, AJKDBlog Contributor, and Abeer Almajali, AJKDBlog Guest Contributor.
To view Wong et al abstract or full-text (subscription required), please visit AJKD.org.
Title: In-Center Nocturnal Hemodialysis Versus Conventional Hemodialysis: A Systematic Review of the Evidence
Authors: B. Wong, D. Collister, M. Muneer, D. Storie, M. Courtney, A. Lloyd, S. Campbell, and R.P. Pauly
DOI: 10.1053/j.ajkd.2017.01.047
Were the studies looking at in-center nocturnal hemodialysis that was taking place 3 nights or 5 nights a week? Or both?