
Role of Donor Pre-Implantation Biopsies in Kidney Transplantation
PathPointers is a new type of blog post that will highlight important everyday teaching points when reviewing kidney histology. These blog posts will be brief and easy-to-read, using real clinical images to demonstrate various biopsy findings. In addition to AJKD Social Media Editor, Timothy Yau, and Education Editor, Stanley Goldfarb, these posts are also reviewed and edited by Pathology Editor, Matt Palmer.
Our kidney transplant program was recently offered the left kidney from a thinly built 26-year-old male donor, who was 5’ 1” (155 cm) tall and weighed 100 lbs (45.4 kg). The donor had died of head trauma. The last available serum creatinine was 3.5 mg/dl. A donor kidney wedge biopsy was performed to evaluate the anatomic integrity of the organ being evaluated for transplantation. Frozen section evaluation was performed within 30 minutes of notification.
As one might have expected from the young age of the donor, there was no interstitial fibrosis, tubular atrophy, arteriosclerosis, arteriolar hyalinosis, or glomerulosclerosis. However, >90% of the kidney was infarcted and showed thrombotic microangiopathy (Figures 1 & 2). The kidney was declined. Thrombotic microangiopathy was attributed to traumatic injury to the brain, which can release thromboplastin-like substances that trigger intravascular coagulation.
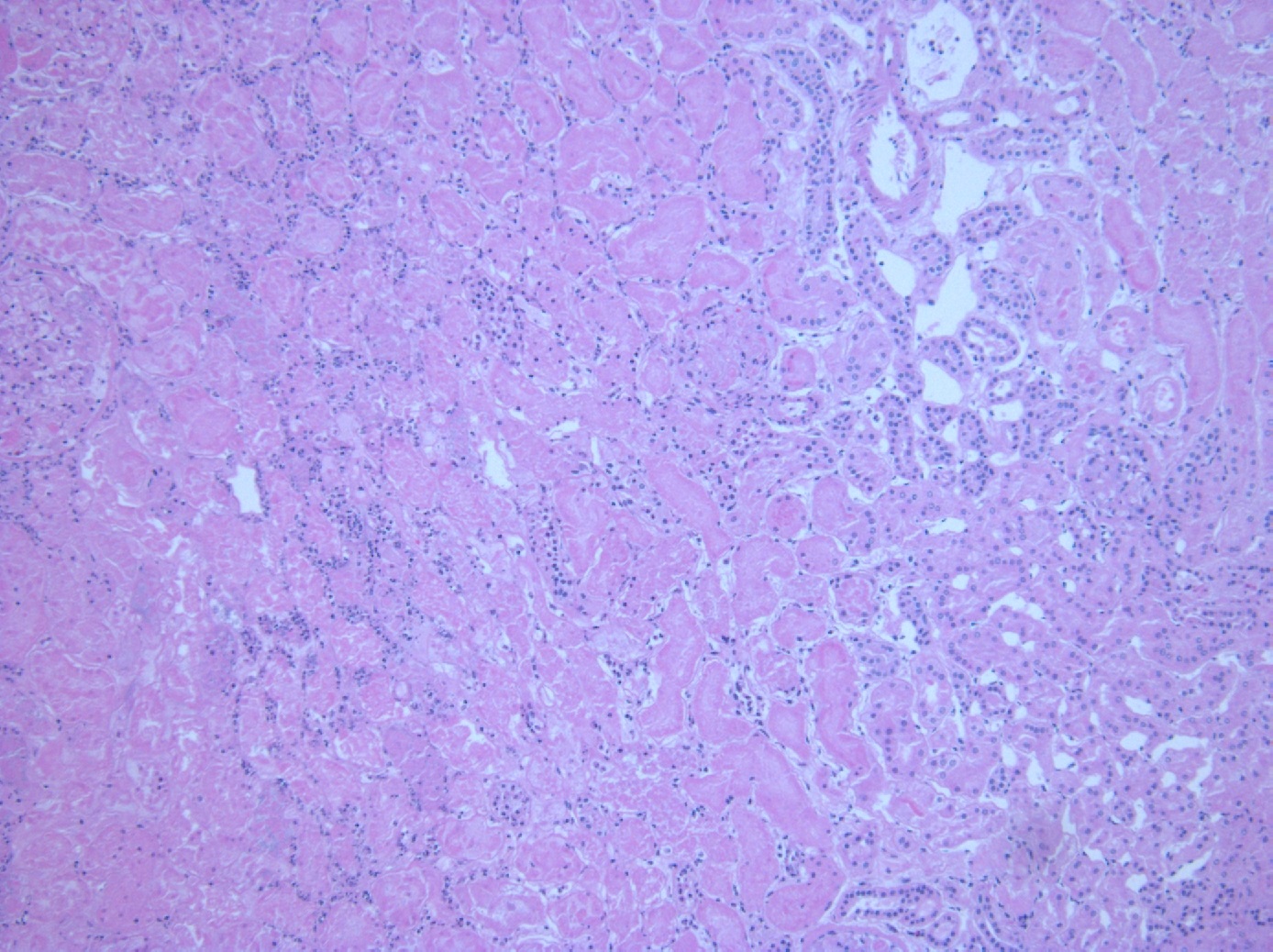
Figure 1. The majority of the renal tubules show coagulative necrosis of the tubules. Only a thin rim of viable parenchyma can be seen on the right side of the photomicrograph.

Figure 2. The glomerulus in this filed is also necrotic. This finding indicates this biopsy should be diagnosed as an acute infarct rather than acute tubular necrosis. Moreover, several glomerular capillaries and arterioles show fresh thrombi, which provide the basis for the diagnosis of thrombotic microangiopathy.
This case illustrates the utility of a donor biopsy in evaluation of organs under consideration for transplantation. In an era of marked organ shortage, there is an increasingly prevalent viewpoint that donor biopsies should be abandoned, as these are associated with increased rates of organ discard. On one hand, situations exist where inappropriate thresholds (eg 20% glomerulosclerosis) may be taken out of context and lead to inappropriate organ discard. However, a properly evaluated biopsy can also prevent transplantation of organs that are unlikely to function post-transplantation. In the current case, the biopsy was able to distinguish between potentially reversible acute kidney injury, and irreversible parenchymal necrosis.
Equally important, a biopsy can expand the donor pool in situations where clinical parameters would raise valid questions about the quality of the organ being offered, such as a history of hypertension and/or diabetes mellitus, or evidence of hepatitis C virus infection. Currently, these donor parameters result in the assignment of a substantial negative clinical score without regard to either duration or severity of disease. Normal histology in this setting may offer justification for proceeding with the transplant.
– Post prepared by Parmjeet Randhawa, AJKDBlog Contributor.
Leave a Reply