
#NKFClinicals 2018: Cancer Drug-Induced AKI
Renal Emergencies in the Cancer Patient: A Case-Based Session (April 13, 2018)
Chair: Mark Perazella
My mentor from residency Perazella talking about chemo induced aki #NKFClinicals pic.twitter.com/WBgWSDjdx4
— Kenar Jhaveri (@kdjhaveri) April 13, 2018
Three classes of agents are generally employed in the treatment of patients with cancer:
- Conventional chemotherapeutic agents
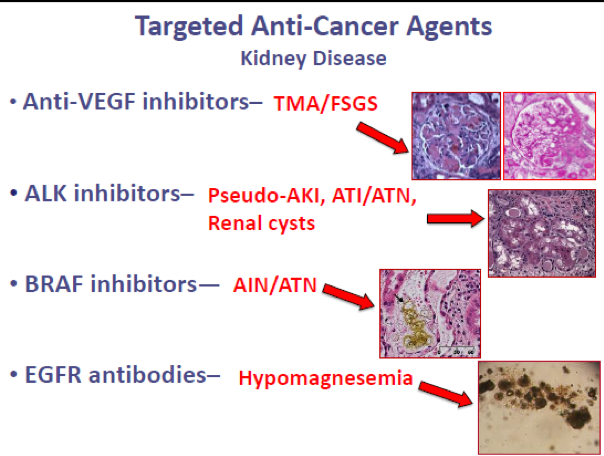
- Targeted anti-cancer therapies
- Cancer immunotherapies
Methotrexate-related renal injury
- Nephrotoxicity occurs with high-dose therapy (1-12 g/m2), rarely with long-term conventional dosing: AKI is primarily from acute tubular injury
- Precipitation of MTX/7-OH MTX crystals in distal tubular lumens
- Direct tubular injury (formation of oxygen radicals associated with adenosine deaminase activity)
- Treatment includes High-flux hemodialysis and Glucarbidase (carboxypeptidase-G2)
- Key reference: Perazella MA and Luciano RL, 2015

Anti-VEGF therapy
- Usually leads to HTN, proteinuria, and TMA. FSGS and MCD have also been reported mainly with Tyrosine kinase inhibitors
- Severe cases of HTN and nephrotic syndrome require treatment changes
- Key reference: Gurevich F and Perazella MA, 2009
Immunotherapy
- Anti-CTLA-4 and PD-1 and PDl1 inhibitors: Classic findings are AIN and, in some cases, rare immune complex GN
- Treatment with steroids usually reverses findings
- Transplant patients can have severe cases of rejection
- Key references: Jhaveri KD and Perazella MA, 2018; Wanchoo R et al, 2017

Chimeric Antigen Receptor T-cells therapy
- This new form of therapy can lead to a cytokine storm and prerenal AKI and some cases of TLS and ATN
- Anti Il-6 agents are used in treatment of the cytokine storm
- Key reference: Jhaveri KD and Rosner MH, 2018
– Post prepared by Kenar Jhaveri, AJKD Social Media Advisory Board member. Follow him @kdjhaveri.
—
The NKF Spring Clinical Meeting abstracts are available in the April 2018 issue of AJKD. Check out more AJKDBlog coverage of #NKFClinicals!
Leave a Reply