
#NephMadness 2025: Resistant Hypertension Region
Submit your picks! | @NephMadness | @nephmadness.bsky.social | NephMadness 2025
Selection Committee Member: Jordana Cohen @jordybc.bsky.social
Jordana Cohen is an Associate Professor of Medicine and Epidemiology in the Renal-Electrolyte and Hypertension Division at the University of Pennsylvania. Her NIH-sponsored research program examines physiology-driven pharmacologic effects of antihypertensive medications in high-risk patients. She is Chair of the American Heart Association’s Hypertension Science Committee and Co-Chair of the American Medical Association’s Blood Pressure Validated Device Listing.
Writer: Stephanie Torres Rodriguez @stephanietr612 — @stephanietr612.bsky.social
Stephanie Torres Rodriguez, M.D., is an Assistant Professor in the Department of Internal Medicine’s Division of Nephrology at UT Southwestern Medical Center. She earned her medical degree at the University of Puerto Rico, where she also completed a residency in internal medicine. She received advanced training in nephrology through a fellowship at UT Southwestern, where she was also Chief Fellow. Her areas of interest are glomerular diseases, POCUS, and medical education.


Competitors for the Resistant Hypertension Region
Team 1: Renal Denervation
versus
Team 2: Novel Drugs for Hypertension
Image generated by Evan Zeitler using DALLE-E 3, accessed via ChatGPT at http://chat.openai.com, February 2025. After using the tool to generate the image, Zeitler and the NephMadness Executive Team reviewed and take full responsibility for the final graphic image.
How many patients in your clinic or hospital setting have hypertension listed as one of their medical diagnoses? I bet there are a lot! The World Health Organization (WHO) estimates that worldwide there are 1.28 billion adults aged 30-79 years with hypertension. In the United States it is the second leading cause of kidney failure and a significant contributor to cardiovascular mortality and morbidity.
Globally, hypertension is the leading preventable and modifiable risk factor for cardiovascular disease, stroke, disability, and premature mortality. Even though hypertension is a common and prevalent disease, this is definitely a topic we should not sleep on, since lives are saved with better blood pressure (BP) control. The WHO estimates that increasing the percentage of controlled hypertension to 50% would prevent 76 million deaths between 2023 and 2050.
Only 21% of individuals diagnosed with hypertension are estimated to have it under control. The reasons for this are multifactorial: limited resources, physician inertia (failure of healthcare providers to initiate or intensify therapy when they encounter BP levels above goal), and adherence, among others.
Resistant hypertension is defined as uncontrolled hypertension despite 3 or 4 antihypertensive drugs of different classes, or controlled BP with 4 or more antihypertensive drugs; both definitions include a thiazide diuretic and all medications at maximally tolerated doses. Resistant hypertension prevalence ranges from 2%-40%, according to various studies.
Before introducing our key players, let’s review the current treatment paradigm and diagnostic approach for managing resistant hypertension. A critical first step in this process is evaluating adherence to the prescribed antihypertensive regimen, as adherence to multi-drug regimens is often challenging. A meta-analysis of 42 studies involving 71,353 patients found that non-adherence in resistant hypertension has a pooled prevalence of 7%. This highlights the need to assess adherence carefully, simplify drug regimens where possible, and prioritize strategies to improve adherence before adding new medications or dose escalation of existing ones.
All patients with resistant hypertension should be worked up for secondary causes. Obstructive sleep apnea, highly prevalent in this population, warrants particular attention, as identifying and evaluating patients for this entity is important as treatment can reduce BP by 5–10 mm Hg. While the exact mechanism is unclear, increased aldosterone via sympathetic stimulation of the adrenals is postulated to be involved. It is also becoming more and more recognized that primary hyperaldosteronism, as reviewed in NephMadness 2019, is exceedingly common and should be assessed by checking plasma aldosterone and plasma renin activity even when hypokalemia and metabolic alkalosis are absent. Selected patients should be assessed for renovascular hypertension (fibromuscular dysplasia in younger women), pheochromocytoma, and Cushing’s syndrome, as well as screening for medications or substances such as NSAIDs, steroids, decongestants, oral contraceptives, illicit drugs (e.g., cocaine, amphetamines), or licorice.
The treatment of resistant hypertension has been a topic of considerable debate, with many opinions but relatively few well-conducted clinical trials to evaluate different strategies. One notable exception is the PATHWAY-2 trial, a double-blind, placebo-controlled crossover study involving 335 adults with resistant hypertension. Participants were defined as having a systolic blood pressure (SBP) >140 mm Hg despite three months of treatment with maximally tolerated doses of three antihypertensive drugs.
Participants were assigned, in a randomized and pre-specified order, to 12-week treatment periods with spironolactone, bisoprolol, doxazosin, or placebo, in addition to their baseline antihypertensive regimen. The primary outcome was the reduction in home SBP (active treatment minus placebo). Spironolactone demonstrated the greatest efficacy, reducing SBP by an average of 10 mm Hg, significantly outperforming doxazosin (5 mm Hg) and bisoprolol (4 mm Hg). Although hyperkalemia was noted with spironolactone, only 2% experienced potassium levels above 6 mmol/L.

Box 1 from Fay and Cohen, © National Kidney Foundation.
How can we help patients with resistant hypertension? What is on the horizon when running out of options? It is time to meet our two teams!
Team 1: Renal Denervation

Copyright: Sergey Novikov/ Shutterstock
Renal denervation is not a new technique or concept; its origins date back nearly 150 years, when a link between the sympathetic nervous system and hypertension was recognized. The kidneys are densely innervated organs which control a variety of kidney functions. The innervation of the kidneys are mainly composed of both efferent (going to the kidneys from the central nervous system [CNS]) sympathetic and afferent (going from the kidneys to the CNS) sensory nerves. These nerves traverse the renal arteries to make their way to the kidney parenchyma.
Increased activity of the efferent sympathetic nervous system contributes to elevated blood pressure through several mechanisms. One primary mechanism involves the stimulation of β1-adrenergic receptors on juxtaglomerular cells, promoting the release of renin. Renin triggers a cascade culminating in the production of angiotensin II (Ang II) and aldosterone, both of which raise blood pressure. Additionally, activation of α-adrenergic receptors on proximal tubule cells enhances the abundance of the Na+/H+ exchanger (NHE), increasing sodium reabsorption and further elevating blood pressure.
Sympathetic stimulation also affects the afferent and efferent arterioles of the glomerulus, causing vasoconstriction that reduces renal blood flow and glomerular filtration rate (GFR), thereby promoting hypertension. Most sensory afferent nerves in the kidney are concentrated in the renal pelvic area, with the highest density in the renal pelvic wall. However, recent evidence has demonstrated sensory nerves traversing all the way to the glomerular capsule. Few afferent nerve fibers are found in the cortex, and they are even scarcer in the medulla. Mechanoreceptors in the renal pelvis detect changes in pelvic pressure caused by urine flow, while two types of chemoreceptors respond to distinct stimuli: Type R1 chemoreceptors are activated by renal ischemia, and Type R2 chemoreceptors sense changes in ionic composition.
Afferent renal nerves transmit sensory information from the kidney to key regions of the CNS involved in cardiovascular regulation, including the paraventricular nucleus (PVN), rostral ventrolateral medulla (RVLM), nucleus tractus solitarius (NTS), preoptic area, subfornical organ, and lateral hypothalamus. This sensory feedback plays a pivotal role in systemic cardiovascular control, contributing to effects such as increased cardiac hypertrophy, elevated peripheral sympathetic tone, and heightened urinary norepinephrine excretion, all of which drive cardiovascular dysfunction.
These afferent nerves likely respond to changes in renal perfusion pressure, ischemia, and injury by transmitting signals that influence central sympathetic outflow. The kidney relies on baroreceptors to detect these physiological changes. Under normal conditions, baroreceptors respond to arterial stretching by signaling the brain to reduce sympathetic outflow, thereby lowering blood pressure.
However, in hypertension, this regulatory mechanism is often disrupted, leading to heightened sympathetic nervous system activity. This hyperactivity is strongly correlated with the severity of hypertension, a phenomenon commonly referred to as neurogenic hypertension. This association underscores the critical role of the sympathetic nervous system in the pathogenesis and progression of hypertension.
This modulation affects systemic vascular resistance and cardiac output, linking kidney sensory input directly to blood pressure regulation and cardiovascular health. Consequently, significant efforts have been directed at modulating this renal-cardiovascular axis to lower blood pressure, improve cardiovascular health, and mitigate the burden of cardiovascular disease.

Prior to the pharmacology era, there were big efforts to explore interventions to interrupt the link between the sympathetic nervous system and hypertension. In 1925, Adson performed the first surgical sympathectomy for the treatment of malignant hypertension. After that, for nearly two decades, this became the procedure of choice for patients with malignant and resistant hypertension. However, in addition to a high surgical mortality, this procedure was associated with major side effects like orthostatic hypotension, impotence, and bowel incontinence. In the mid 1950’s the pharmacologic era started and the practice of sympathectomy was abandoned.
Research efforts to deepen our understanding of the relationship between the sympathetic nervous system and hypertension have persisted over the years. Particular attention has been given to exploring the connection between the renal sympathetic system and the development and progression of hypertension. Various experimental animal models showed that the renal sympathetic nerves (which lie within and adjacent to the renal arteries) are key players in neurogenic hypertension’s pathophysiology.
The first studies
In 2007, the first catheter-based renal denervation technique was performed. Soon after, in 2009, Symplicity HTN-1 was published, marking the first evaluation of the efficacy and safety of this technique for resistant hypertension. The study showed a significant reduction in office blood pressure- 22 mm Hg in systolic and 11 mm Hg in diastolic – at 6 months that was sustained after 1 year. However, no sham control group was included in this study.
Symplicity HTN-2 study followed in 2010 as the first randomized controlled trial with the inclusion of a control group (but no procedure sham), and it was not blinded. It resulted in no change in blood pressure in the control group, but significant reduction in office blood pressure in the renal denervation group. Six months after the intervention, the systolic blood pressure was reduced by 32 mm Hg and diastolic by 12 mm Hg.
The excitement about renal denervation grew exponentially with this encouraging data. It led to the development of other catheter-based devices and the approval of this procedure for clinical use in Europe by 2012. However, there was skepticism about the already published data. Some of the critiques were: no assessment of ambulatory blood pressure, small sample sizes, suboptimal antihypertensive therapy, and lack of a sham control group (sham procedure: a simulated medical procedure that mimics an active procedure).
Stronger evidence was required for the approval of renal denervation by the FDA in the United States. To address previous critiques, the Symplicity HTN-3 trial was conducted and was published in the the New England Journal of Medicine in 2014. This was the first large-scale (535 patients randomized 2:1), prospective, sham-controlled study on renal denervation. However, the trial failed to achieve its primary efficacy endpoint. After six months, the reduction in office systolic blood pressure was 14 mm Hg in the renal denervation group compared to 12 mm Hg in the sham-control group, resulting in a non-significant difference of just 2 mm Hg between the groups.
The results of Symplicity HTN-3 reignited skepticism, casting doubt on the effectiveness of renal denervation for patients with resistant hypertension. Proponents of the technique challenged the validity of the trial’s findings, citing concerns that the standardized renal denervation procedure used in the study may have been insufficiently aggressive, limiting its efficacy. Additionally, of the 111 interventionalists involved, 60 had performed only two or fewer renal denervation procedures, raising doubt about operator expertise and consistency. Changes in medication usage during the trial further complicated the interpretation of results, potentially masking the true effect of renal denervation.
Following the dampened excitement surrounding renal denervation due to the Symplicity HTN-3 results, there has been a renewed focus on improving the renal denervation technique, and more studies have been performed in an effort to address the issues stemming from the Symplicity HTN-3 controversy.
Currently, three novel techniques for renal denervation have been developed, two of which are approved: radiofrequency ablation and ultrasound ablation. The third, the dehydrated alcohol injection technique, is still under development.
- Symplicity Spyral System (Medtronic): This FDA approved device delivers a medium-frequency alternating current via a catheter with 4 electrodes arranged in a spiral sequence. The electrodes generate only enough heat to destroy the nerves in the renal artery periadventitial space, without injuring the arterial wall.
- Paradise System (Recor Medical): This FDA approved device uses a catheter with an inflatable balloon system to deliver ultrasound energy to the main renal arteries while simultaneously irrigating the lumen of the vessel with a cooling solution. The solution maintains a lower temperature within the renal artery and prevents injury to the arterial wall.
- Peregrine System (Ablative Solutions): This device uses a catheter with three embedded, concentrically placed microneedles. The needles pass through the renal artery into the perivascular space before releasing small amounts of dehydrated alcohol to treat the renal nerves.
Radiofrequency ablation
The Symplicity Spyral System (Medtronic) employs a multi-electrode catheter designed to deliver circumferential ablation in a spiral pattern, targeting four quadrants of the renal artery and its branch vessels. This approach has been evaluated in two important clinical trials: SPYRAL HTN OFF-MED, and SPYRAL HTN ON-MED.

SPYRAL HTN OFF-MED Pivotal trial was a multi-center, international, prospective, single-blind, randomized, sham-controlled study. The trial design attempted to overcome issues with inadequate nerve ablation and diminish concerns about anti-hypertensive medication imbalances between the groups. The study enrolled patients with resistant hypertension who had a mean 24-hour systolic blood pressure of at least 140 mm Hg but less than 170 mm Hg, as measured by ambulatory blood pressure monitoring while being completely off all antihypertensive medications.
The primary endpoint was the change in mean 24-hour systolic blood pressure from baseline to three months post-procedure. They chose three months to minimize the duration of time off antihypertensive meds. The trial demonstrated a modest but significant treatment difference of -4 mm Hg in favor of the renal denervation group compared to the sham procedure group. Importantly, this benefit was achieved with a favorable safety profile, as no major safety events were reported within the first month following the procedure.
Investigators suggest that the modest reduction in systolic blood pressure observed in the trial may be attributed to the relatively short follow-up period, with the potential for a greater effect had the trial extended to six months. Additionally, it is important to note that, by the three-month mark, 9% of patients in the renal denervation group and 5% in the sham-control group were taking antihypertensive medications despite not meeting the study’s escape criteria—the only condition under which such medications were permitted.
Moreover, the exclusion of patients with heart failure, cerebrovascular accidents, transient ischemic attacks, or atrial fibrillation further limits the generalizability of the study findings to broader patient populations. These factors highlight the need for longer follow-up and more inclusive study designs to fully assess the efficacy and applicability of renal denervation.
OFF-MED set the stage for testing the effect of renal denervation in patients who continued anti-hypertensive medications. Next up, the SPYRAL HTN ON-MED trial was set to answer that question. This is a global, randomized, blinded, sham-controlled trial with the same inclusion criteria as SPYRAL HTN OFF-MED trial, but these patients had to be taking up to three antihypertensive medications. The primary endpoint was the treatment difference in mean 24-hour systolic blood pressure at 6 months between the renal denervation group and the sham control group. At 6 months, there was a decrease of 24-hour ambulatory systolic blood pressure of 9 mm Hg in the renal denervation group and 2 mm Hg in the sham-controlled group for a significant adjusted difference between groups of 7 mm Hg favoring renal denervation. The main limitations of this study are the small sample size and variable adherence to anti-hypertensive medications, which was approximately 60%.
These favorable results were challenged by the findings in the SPYRAL HTN ON-MED Expansion Trial. Despite an increase in the total sample size to 257 patients, it did not meet the primary efficacy endpoint. The change in 24-hour ambulatory systolic blood pressure in the renal denervation group was a decrease of 6.5 mm Hg and a decrease of 4.5 mm Hg in the sham-controlled group for a non-significant difference of 2 mm Hg. Despite these issues, the Spyral system was narrowly approved by the FDA in 2023.
Ultrasound-based ablation
Let’s shift gears now and explore the second type of renal denervation technique: ultrasound ablation. This technique is designed to deliver a minimum of two sonications of 7 seconds each, separated longitudinally by 5 mm in the main renal arteries. Three trials have explored this technique: RADIANCE-HTN SOLO, RADIANCE-HTN TRIO, and RADIANCE II.

RADIANCE-HTN SOLO is a multi-center, international, single-blind, randomized, sham-controlled trial. Patients with a history of cardiovascular or cerebrovascular events, or eGFR less than 40 mL/min/1.73m2 were excluded. Patients who met eligibility criteria had blood pressure meds held for 2 months after the procedure with a protocol for escape if office blood pressures were >180/110 mm Hg or home blood pressures >170/105 mm Hg. The primary effectiveness endpoint was the change in daytime ambulatory systolic blood pressure at 2 months in the intention-to-treat group. Results showed a greater decrease in daytime ambulatory systolic blood pressure at 2 months in the renal denervation group (-8 mm Hg) versus the sham procedure group (-2 mm Hg), with a significant difference of -6 mm Hg between groups with no safety events. It also showed that 20% of patients in the renal denervation group were able to have daytime ambulatory blood pressures of less than 135/85 mm Hg without any anti-hypertensive medications versus 3% on the sham procedure group (p=0.001).
RADIANCE-HTN TRIO, in contrast with RADIANCE-HTN SOLO, included patients with resistant hypertension defined as office systolic blood pressure of at least 140 mm Hg and diastolic blood pressure of at least 90 mm Hg despite being on a stable regimen of three or more anti-hypertensive medications, one of them being a diuretic. All participants were continued on a standardized protocol (amlodipine 10 mg or 5 mg in the event of leg edema), valsartan 160 mg (or olmesartan 40 mg), and hydrochlorothiazide 25 mg. No other antihypertensive medications were allowed except β blockers for chronic coronary syndrome or heart failure. This study showed a median in between groups systolic blood pressure difference of -4.5 mm Hg (95%CI -8.5 to -0.03). Three major adverse events were reported; only one was procedure related which was an access site pseudoaneurysm, and it was treated successfully.
RADIANCE II trial recruited patients that met these three criteria:
- Uncontrolled hypertension was defined as seated office SBP/DBP >140/90 mm Hg but less than 180/120 mm Hg while taking up to two antihypertensive medications of different classes.
- No history of cardiovascular or cerebrovascular events.
- eGFR > 40 mL/min/1.73m2
Similar to RADIANCE-HTN SOLO, antihypertensive medications were held for 2 months post-denervation with similar escape parameters. The primary efficacy outcome was the mean change in daytime ambulatory SBP at 2 months. The results showed a baseline adjusted between-group difference of -6.3 mm Hg (95%CI -9.3 to -3.2, p=<0.001), which were very similar to the RADIANCE-HTN SOLO results.
The positive results of the published trials post-Symplicity HTN-3 led to the FDA approval of two renal denervation device systems in November 2023: Symplicity Spyral Renal Denervation System (radioablation technique) and the Paradise Ultrasound Renal Denervation System.
While these findings represent a significant step forward for renal denervation, it is important to critically evaluate the trial results. Across studies, the observed reductions in systolic blood pressure have been modest. For context, a single antihypertensive medication can achieve a comparable reduction of approximately 5 mm Hg. This raises the question: is it worth undergoing an invasive procedure to achieve results similar to those of a single medication, especially when the effect of the procedure is not guaranteed?
That said, renal denervation does offer potential advantages, particularly in addressing challenges with medication adherence. As a longer-term intervention, it may benefit patients who struggle to maintain consistent use of antihypertensive drugs from side effects or adherence. However, concerns remain about the potential for nerve regeneration, which could diminish the procedure’s efficacy over time. Lastly, the majority of trials included no patients with significant chronic kidney disease and the ultrasound ablation studies performed by the Paradise System excluded those with eGFR <40. The global SYMPLICITY registry data showed that patients with CKD (defined as an eGFR <60 but >15) had comparable reductions in blood pressure to those without CKD. However, these are not data from randomized trials. It remains to be seen how this group will benefit from this procedure. Further research is needed to clarify these uncertainties and establish the role of renal denervation in managing resistant hypertension.
Another important observation is that, despite some of these trials achieving statistically significant differences between the renal denervation group and the sham-controlled group, we must ask: is this difference clinically significant? It must be pointed out that modest blood pressure reductions in the ~5 to 10 mm Hg range in clinical trials can result in meaningful decreases in clinical outcomes. All of the trials mentioned here reported a reduction in systolic blood pressure in the sham-controlled group ranging from 0.6 to 4.5 mm Hg. That’s quite a good placebo effect, right? Again, is it worth undergoing the procedure when the placebo effect can be almost as effective?
Nevertheless, what do patients think about renal denervation intervention? A retrospective survey data analysis attempted to answer this question. This study found no relationship between a patient’s current blood pressure level and their willingness to consider a renal denervation procedure. Similarly, there was no association between the number of antihypertensive medications a patient was taking and their attitude toward the procedure. Patients more inclined to consider renal denervation were those who perceived hypertension as a significant health problem or had experienced side effects from their antihypertensive medications. Another factor influencing willingness was the presence of comorbidities; patients with a higher number of comorbid conditions were more likely to prefer renal denervation over medication-based treatments. What about a patient’s readiness for renal denervation procedure? The study also revealed that the single most influential factor in a patient’s willingness to undergo renal denervation was their physician’s recommendation. Another significant motivator was the promise of reduced blood pressure following the procedure. However, this expectation poses a potential challenge, as renal denervation does not guarantee effectiveness for every patient. This underscores the critical need for transparent and thorough physician-patient discussions about the risks, benefits, and realistic outcomes of the procedure. Managing patient expectations is essential to ensure informed decision-making and alignment with individual treatment goals.
Renal denervation has demonstrated a strong safety profile in clinical trial settings with minimal adverse effects, but it remains an uncertain intervention. There is currently no way to predict its immediate effectiveness or guarantee a reduction in medication burden after the procedure. Despite these uncertainties, its safety may make it a viable option for selective patients, particularly those dealing with polypharmacy or significant side effects from antihypertensive medications. In addition, a cost-effectiveness analysis projected that catheter based renal denervation is a high value and cost-effective intervention, estimating a $32,732 incremental cost-effectiveness ratio per quality adjusted life years gained over lifetime. This surpasses the estimated intervention cost of approximately $20,000.
Many critical questions remain unanswered. Who stands to benefit most from renal denervation? While it may be safe, does its cost justify its use for a procedure with no guaranteed effect? And the overarching question persists: is it truly worth it? As an example, the addition of spironolactone at 25 mg per day can reduce blood pressure even more with a fraction of the cost. Granted, you have to take the medicine and consider the side effects. Addressing these uncertainties will be key to defining the role of renal denervation in the management of hypertension.
In this podcast episode of The Curbsiders hosts Matt Watto and Paul Williams are joined by Jordy Cohen:
#474 Resistant Hypertension the Next Frontier
Team 2: Novel Rx for HTN

Copyright: Grandomart/ Shutterstock
The renin-angiotensin-aldosterone system (RAAS) is a primary target for the most widely used classes of antihypertensive medications: angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), mineralocorticoid receptor antagonists (MRAs), and direct renin inhibitors.
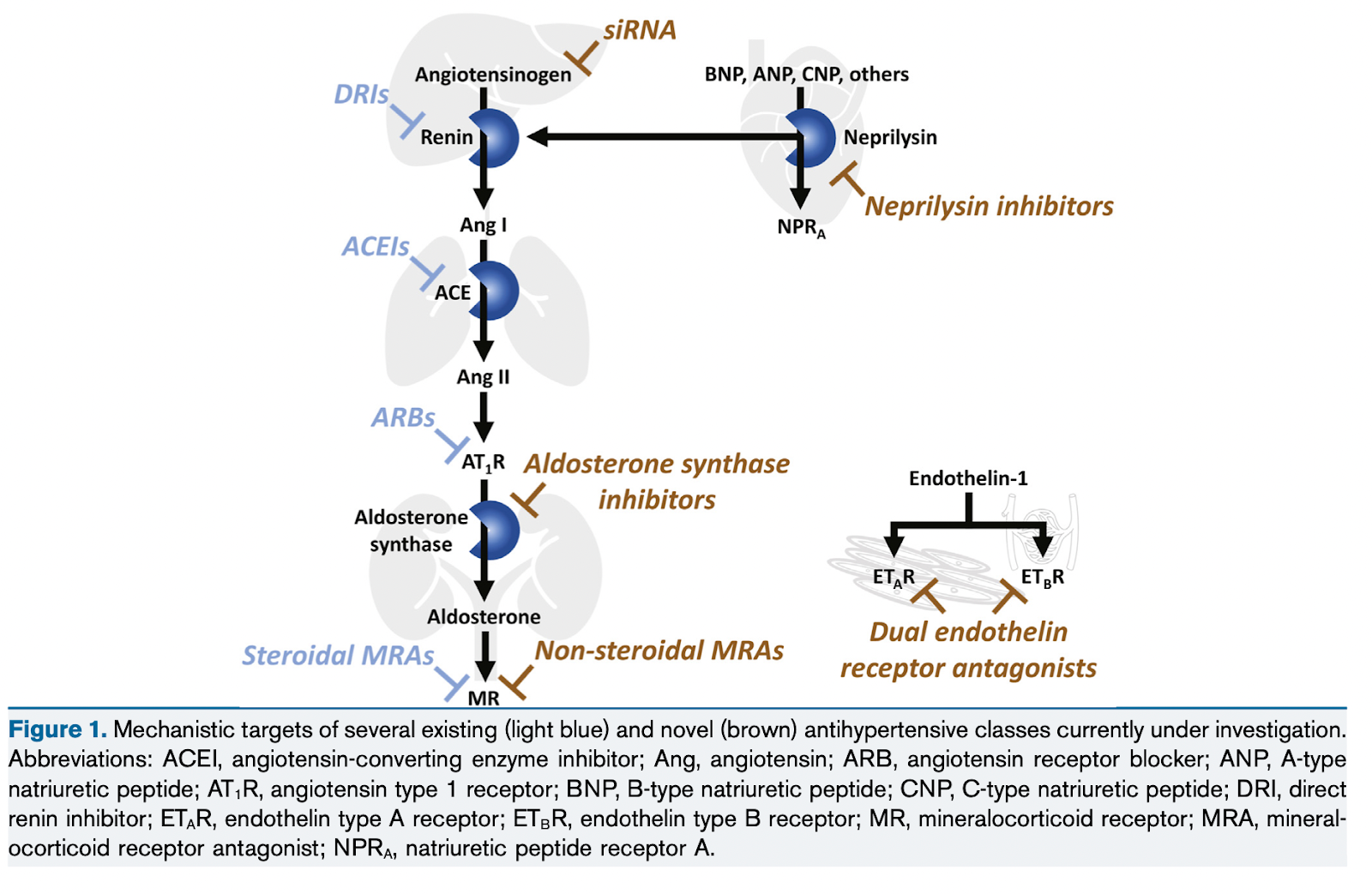
Mechanistic targets of several existing (light blue) and novel (brown) antihypertensive classes currently under investigation. Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; Ang, angiotensin; ARB, angiotensin receptor blocker; ANP, A-type natriuretic peptide; AT1R, angiotensin type 1 receptor; BNP, B-type natriuretic peptide; CNP, C-type natriuretic peptide; DRI, direct renin inhibitor; ETAR, endothelin type A receptor; ETBR, endothelin type B receptor; MR, mineralocorticoid receptor; MRA, mineralocorticoid receptor antagonist; NPRA, natriuretic peptide receptor A. Figure 1 from Cohen et al, © National Kidney Foundation.
Despite the availability of multiple drugs targeting different parts of the RAAS, contributors like inadequate systemic and renal vasodilation, inflammation, endothelial dysfunction, and aldosterone excess continue to pose challenges in adequate treatment of resistant hypertension. A notable issue is the “aldosterone escape,” where angiotensin II and aldosterone levels rebound after an initial suppression. These limitations have opened the doors to look at other targets like aldosterone synthase and angiotensinogen.
The endothelin system, particularly endothelin-1 produced by the vascular endothelium, also plays a critical role in resistant hypertension. Endothelin-1 regulates vascular tone, promoting vasoconstriction, vascular remodeling, and hypertrophy. It also enhances the production of growth factors and inflammatory mediators ultimately causing hypertension, atherosclerosis, fibrosis, and vascular damage. Endothelin-1 expression is upregulated in severe hypertension, obesity, and CKD.
Now it is time to meet the players on this team.
Dual endothelin receptor antagonist: aprocitentan
Endothelin-1, first identified in 1988, is the most potent vasoconstrictor in the human body. Its actions are mediated through two receptor subtypes: ETA and ETB (subdivided into ETB1 and ETB2). Vasoconstriction occurs primarily when endothelin-1 activates ETA and ETB2 receptors, while vasodilation is triggered by ETB1 receptor activation on endothelial cells. ETB receptor activation on endothelial cells promotes vasodilation and natriuresis via nitric oxide and prostacyclin release, whereas ETB receptor activation on renal tubular cells enhances sodium and water reabsorption. Excessive ETB receptor activation can disturb this balance, leading to fluid retention and edema. ETB receptor-mediated increases in vascular permeability may further contribute to edema formation. These effects serve as a counterregulatory mechanism to limit vasoconstriction and maintain homeostasis. Given ET receptor overexpression in hypertension and kidney diseases, ET receptor antagonists have been extensively studied over the past three decades as potential therapeutic agents.
The first human study evaluating the effects of ET receptor antagonists was conducted in 1998 using bosentan, a dual ETA and ETB receptor antagonist. Bosentan administration significantly reduced office systolic and diastolic BP compared to placebo. However, its use was associated with notable adverse effects, including headache, flushing, lower extremity edema, and increases in liver enzymes, raising concerns about its hepatic safety. Bosentan received FDA approval for pulmonary hypertension but not for arterial hypertension. Similar outcomes and adverse effects were observed with darusentan, a selective ETA receptor antagonist, highlighting the challenges of balancing efficacy with tolerability in this drug class.
Due to persistent side effects, it was suggested that this therapeutic approach may not be beneficial for most people with hypertension but only for specific patients, like those with resistant hypertension.
In an attempt to seek the same effective results, but with a better safety profile, we call in our first player, aprocitentan.

Aprocitentan, a potent dual ETA and ETB receptor antagonist, with a long half-life (44 hours) and CYP450 independent metabolism, was studied in the PRECISION trial. Among 730 adults with resistant hypertension, aprocitentan reduced office SBP by 15 mm Hg at 4 weeks in both the 12.5 mg and 25 mg dose groups compared to 11 mm Hg with placebo, with greater efficacy in older patients and those with macroalbuminuria or CKD stages 3–4. Another unique finding is that aprocitentan has a higher blood pressure lowering effect at night time with a decrease in SBP of 5.1 mm Hg and 7.4 mm Hg compared to daytime, with a decrease in SBP of 3.8 mm Hg and 5.3 mm Hg for 12.5 mg and 25 mg doses, respectively. Hepatotoxicity was rare (2.3% in the 25 mg group). Fluid retention/edema, the most common adverse effect, was dose-dependent, affecting 18% of patients by 4–6 weeks and persisting at 32 weeks. Thirteen patients discontinued treatment due to edema, and 11 were hospitalized for heart failure exacerbation. The authors recommend close follow-up and diuretic adjustment during the first 4 weeks. Despite this, aprocitentan is the first FDA-approved dual endothelin receptor antagonist for resistant hypertension. Will it revolutionize treatment? Time will tell.
Aldosterone synthase (CYP11B2) inhibitor: baxdrostat & lorundrostat
In an attempt to bypass the aldosterone escape effect, aldosterone synthase became a target of interest. However, this needed to be very specific to avoid blocking other adrenal pathways, specifically cortisol synthesis. For this, we call our second and third players, the aldosterone synthase (CYP11B2) inhibitors: baxdrostat and lorundrostat.

BrigHTN is a phase 2 trial conducted at community-based practices in the U.S. It excluded patients with blood pressures above 180/110 mm Hg, eGFR less than 45 mL/minute/1.73m2, and uncontrolled diabetes.
The trial showed dose-dependent reductions in mean seated SBP: -20.3 mm Hg (2 mg), -17.5 mm Hg (1 mg), and -12.1 mm Hg (0.5 mg). When compared to placebo, the differences were only significant in the higher doses: -11.0 mm Hg in the 2 mg and -8.1 mm Hg in the 1 mg group.
Adverse events included urinary tract infections, headache, fatigue, and hyperkalemia, but potassium levels normalized with dietary management, and patients were able to complete the trial. There were no instances of adrenocortical insufficiency.
Importantly, baxdrostat showed decreased urinary aldosterone levels and plasma renin activity in all three doses. No reduction in serum cortisol was seen. It is expected that in contrast to mineralocorticoid receptor antagonists, this aldosterone synthase inhibitor will prevent the activation of both genomic and non-genomic pathways which could contribute to vascular smooth muscle cell hypertrophy, vascular fibrosis, and interstitial fibrosis of the kidneys.
The efficacy of lorundrostat for uncontrolled hypertension was tested in the Target-HTN trial. This phase 2 trial divided the participants with resistant hypertension in two cohorts: cohort 1 participants had a plasma renin activity <1.0 ng/mL/hr and serum aldosterone level > 1.0 ng/dL; cohort 2 participants had plasma renin activity > 1.0 ng/mL/hr.
For cohort 1, randomization was 1:1:1:1:1:1 ratio to placebo or 1 of the 5 lorundrostat doses: 12.5 mg, 50 mg, or 100 mg daily or 12.5 mg or 25 mg twice daily. Cohort 2 was randomized to placebo or lorundrostat 100mg daily in a 1:6 ratio.
The primary endpoint resulted in a decrease of mean systolic automated office blood pressure (AOBP) in cohort 1 as follows: 5.6 mm Hg, 13.7 mm Hg, and 11.9 mm Hg corresponding to the 12.5 mg, 50 mg, and 100 mg once daily doses, respectively. These are compared to the decrease in mean systolic AOBP of 4.1 mm Hg in the placebo group. However, the trial showed a similar decrease in mean systolic AOBP between the patients taking lorundrostat 100 mg daily from cohort 2 (11.4 mm Hg) versus cohort 1 (11.9 mm Hg).
All doses of lorundrostat resulted in reduction of serum aldosterone. Notably there were also declines in eGFR parallel to the reduction in systolic AOBP which is consistent with lowering of intraglomerular pressures.
Most adverse events were mild and no adrenocortical insufficiency was reported. Six participants had hyperkalemia with serum potassium levels > 6 mmol/L that improved with dose reduction or drug discontinuation without additional interventions.
More to come about baxdrostat and lorundrostat as the phase 3 trial results are expected in late 2025.
Small interfering RNA (siRNA) for angiotensinogen: zilebesiran
What if I tell you that there is a medication that could keep your blood pressure well controlled and you only need to use it quarterly or twice a year? Sign me up! Back to the future, we call our rookie of the year: zilebesiran.
This medication is an investigational siRNA that binds with high affinity to the hepatic asialoglycoprotein receptor, decreasing hepatic angiotensinogen messenger RNA (mRNA) levels, thus reducing the production of angiotensinogen.
Zilebesiran was studied in a four-part, multi-center, phase 1 trial to assess its safety, and pharmacokinetic and pharmacodynamic characteristics.The report presents data from Parts A, B, & E.
This was a double-blind, randomized, placebo-controlled trial, evaluating a single ascending dose of subcutaneous zilebesiran (10-800 mg) or placebo. This trial found dose-dependent reductions in serum angiotensinogen levels and sustained decreases in 24-hour ambulatory blood pressure for up to 24 weeks with doses of 200 mg or above. Systolic BP decreased by > 10 mm Hg, while diastolic BP decreased by > 5 mm Hg by week 8. A sustained effect by week 24 and a larger BP reduction was observed with the 800 mg dose (-23 mm Hg SBP and -11 mm Hg in DBP).
Zilebesiran was safe, with the most common adverse events being headaches, injection-site reactions, and upper respiratory tract infections. No clinically significant changes in serum potassium, creatinine, or eGFR were reported. There were no deaths or unplanned hospitalizations.
Notably, part B revealed that a high salt intake can reverse the effects of zilebesiran on BP.

Other studies have also evaluated the effect of this medication. The KARDIA-1 trial, a phase 2 study, investigated the effectiveness and safety of zilebesiran in adults with mild to moderate hypertension. Participants received subcutaneous doses of zilebesiran (150 mg, 300 mg, or 600 mg every 6 months, or 300 mg every 3 months) or placebo. After 3 months, zilebesiran reduced the 24-hour average systolic blood pressure by 7.3 to 10.0 mm Hg, while placebo led to a 6.8 mm Hg increase. Adverse events were noted in 60.9% of those receiving zilebesiran compared to 50.7% on placebo, with the most common being mild hyperkalemia and injection site reactions.
Long-acting and effective drugs like zilebesiran can certainly revolutionize the treatment of hypertension. We will stay tuned for more trials on this drug!
Glucagon-like peptide-1 receptor agonist (GLP-1 RA): semaglutide
Yes, you are reading correctly, our last player of this team is GLP-1 RA: semaglutide. (I bet the Gila monster will be very happy about this.)
A meta-analysis of three randomized controlled trials (RCTs) and 3136 participants examined the effect of semaglutide 2.4 mg weekly on systolic blood pressure in patients with hypertension, including resistant hypertension (3.5% of participants).
Over 68 weeks, semaglutide reduced systolic blood pressure by -4.89 mm Hg compared to placebo, with consistent results across subgroups (e.g., systolic blood pressure >130 mm Hg: -5.05 mm Hg). The effect on resistant hypertension (-4.93 mm Hg) was not statistically significant. Notably, semaglutide led to the de-escalation of antihypertensive therapy in 27% of participants compared to 3% in the placebo group. In addition, in this same group, 36% of those treated with semaglutide did not meet resistant hypertension criteria at the end of the study.
A look into the “now” and into the future; these novel drugs for resistant hypertension have some promise and hopefully we continue to see positive data from further studies.
COMMENTARY BY Swapnil Hiremath:
Renal Denervation in Hypertension: Fad or Fixture?
– Executive Team Members for this region: Matt Sparks @Nephro_Sparks – @nephrosparks.bsky.social and Elena Cervantes @Elena_Cervants | Meet the Gamemakers
How to Claim CME and MOC
US-based physicians can earn 1.0 CME credit and 1.0 MOC per region through NKF PERC (detailed instructions here). The CME and MOC activity will expire on June 1, 2025.
Leave a Reply