
Response to Rituximab as a Maintenance Therapy in Adult INS: An Interview
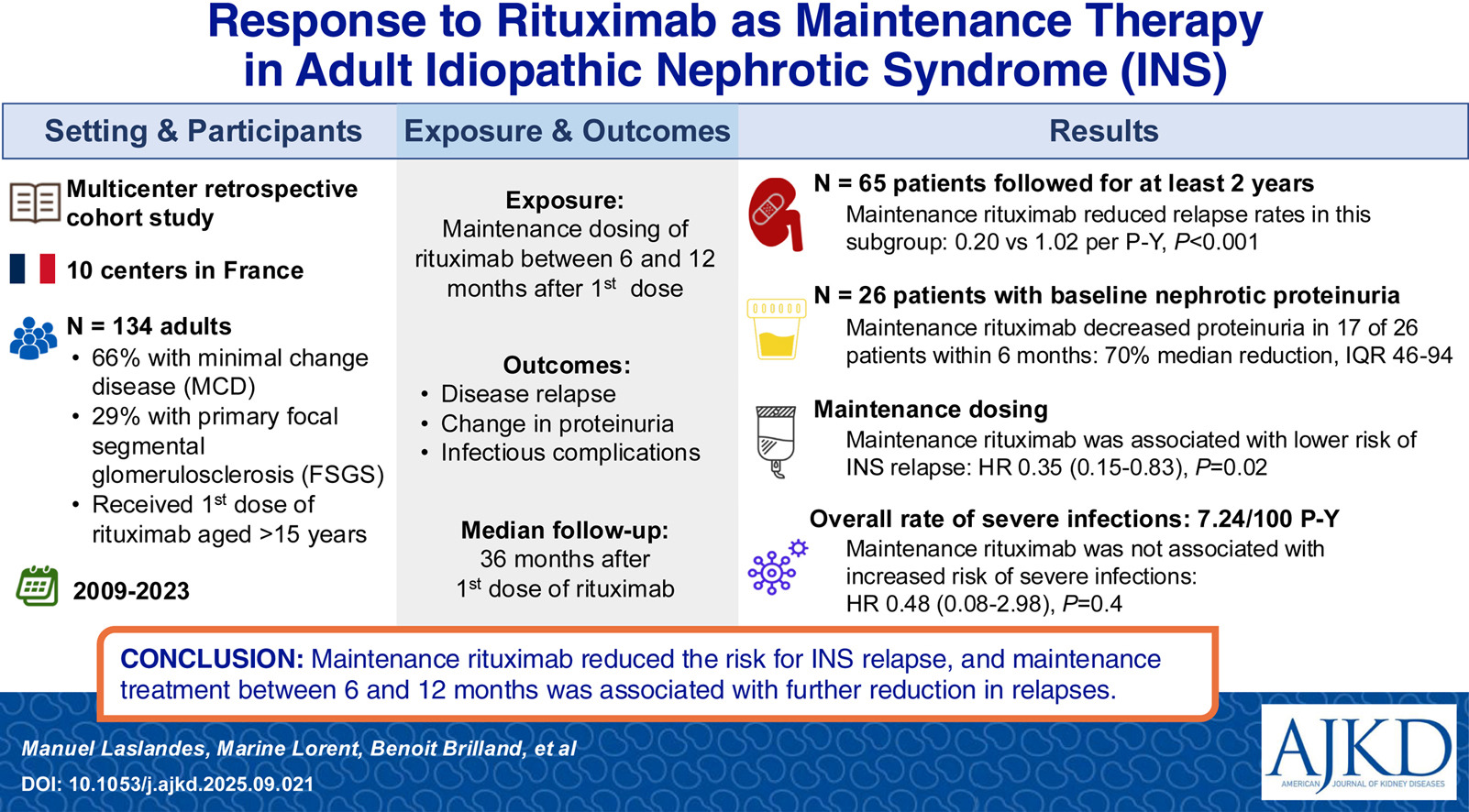
Rituximab effectively limits the number of relapses in childhood idiopathic nephrotic syndromes (INS) and reduces exposure to corticosteroids and other immunosuppressants. However, few data are available on the risk of relapse after an initial dose of rituximab or the benefit of a maintenance therapy in adults with INS. Laslandes et al followed 134 French adults for a median of 36 months to test its effectiveness. AJKDBlog’s Interviews Editor, Timothy Yau (@Maximal_Change), recently sat down with two of the authors of the study, Manuel Laslandes and Christophe Masset, to discuss the implications of their research.
Dr. Manuel Laslandes is a junior nephrologist at Nantes University Hospital, working in the Nephrology and Transplantation Department (Institut de Transplantation Urologie et Néphrologie – ITUN). His clinical and research interests focus on idiopathic nephrotic syndromes and their management, kidney transplantation, and coagulation disorders in kidney disease.
Dr. Christophe Masset is a senior nephrologist currently working in the Nephrology and Transplantation Department at Nantes University Hospital (Institut de Transplantation Urologie et Néphrologie – ITUN). He holds a PhD in basic immunology, and his research focuses on immune diseases in nephrology, with a particular emphasis on autoimmune diseases and kidney/pancreas transplantation. He is also actively involved in the scientific committee of the French network of kidney transplant recipients (DIVAT), enabling translational and large-scale cohort studies.

AJKD Blog: Thank you for publishing this article. In your introduction, you mention that diseases like minimal change disease (MCD) and focal segmental glomerulosclerosis (FSGS) have historically been thought to be T-cell mediated, which explains the response to medications like systemic glucocorticoids. Before we dive into your study, can you summarize the role of a B-cell therapy like rituximab in treating diseases like MCD and FSGS?
AUTHORS: Historically, idiopathic nephrotic syndromes (INS) were primarily thought to be T-cell–mediated diseases. One of the main proponents of this hypothesis was Robert Shalhoub, who outlined several arguments supporting this concept in 1974. His observations were later supported by additional findings, including the efficacy of levamisole and experimental data, such as proteinuria induction in Wistar rats injected with supernatant from T-cell hybridomas derived from patients with MCD.
However, the role of B cells is now increasingly recognized. Several observations have strengthened this hypothesis, ranging from the expansion of memory B cells during disease relapses to the more recent discovery of anti-nephrin antibodies. Following the serendipitous observation that rituximab (RTX) could induce remission in INS, numerous retrospective and prospective studies, particularly in pediatric populations, have demonstrated its potential efficacy.
Initially, RTX was mainly considered a second-line immunosuppressive therapy. Patients with frequently relapsing or steroid-dependent INS were typically treated first with calcineurin inhibitors (CNIs) or mycophenolate mofetil/mycophenolic acid (MMF). RTX was generally reserved for cases of intolerance, adverse effects, or dependence to these agents. Today, however, an increasing number of nephrologists are using it earlier in the disease course, sometimes starting at the first relapses, even before introducing CNIs or MMF.
AJKD Blog: It seems there has been very limited data from earlier studies looking at the risk of relapse when using RTX for INS in adults. What data exist on how it compares to traditional therapies like steroids, and what did you hope to answer when designing your study?
AUTHORS: INS are rare, with a higher incidence in children. As a result, most of the available evidence comes from pediatric studies. For example, the group led by Pietro Ravani conducted a randomized study in 44 children with steroid-dependent disease comparing RTX with a standard-treatment arm in which steroids and CNIs were continued at usual doses. At 3 months, the probability of relapse was significantly higher in the standard-treatment group (48% vs 18%).
Another important pediatric trial led by Kazumoto Iijima evaluated RTX versus placebo in children with steroid-dependent or frequently relapsing disease. The median relapse-free survival increased significantly, from 101 days in the placebo group to 267 days in the treatment group.
Rituximab has also been compared with tacrolimus for maintaining remission in the randomized pediatric RITURNS trial. In that study, the primary endpoint of relapse-free survival at 12 months was significantly higher in the RTX group (90% vs 63.3%).
In adults, however, the available data are much more limited and mostly come from observational studies. A retrospective analysis by Heybeli compared several second-line strategies in adults with frequently relapsing or steroid-dependent minimal change disease, including RTX, MMF, CNIs, and cyclophosphamide. In that study, the median time to relapse after treatment initiation was not significantly different between RTX and the other therapies.
When we started our study in 2020, evidence on RTX use in adults was quite limited. We had the impression in clinical practice that RTX was not only effective in allowing steroid withdrawal, but might also contribute to maintaining long-term remission. Particularly, the question of preventive reinjection – similar to other nephrologic immune diseases using anti B-cell therapies – seemed of great interest, with a large heterogenicity amongst clinical practices. Thus, we aimed to provide valuable data on the use of RTX in INS adults to inform future clinical decisions.
AJKD Blog: Can you tell us about the cohort you studied? In particular, I’m interested in the division of primary glomerular disease (MCD vs FSGS) and how RTX fits into the treatment protocol for these patients.
AUTHORS: We had the chance to rely on a strong collaborative network, which is part of the “Société de Néphrologie de l’Ouest” (literally “the Nephrology Society of West of France”). Here we want to take the opportunity to thank again all our collaborators, that helped us identify patients, finally leading to a unique cohort of 134 adult INS patients – a large number considering published series. The cohort consisted mainly of young adults, with a median age of 37 years at the time of the first RTX administration, and were followed for a median time of 36 months after the first injection.
Due to its retrospective aspect, we observed a certain heterogeneity in RTX use which reflects real-life practices, which allowed us to explore several facets of its use. At the time of the first infusion, 78% of patients were already in complete/partial remission, meaning RTX was primarily used as maintenance therapy, while about 15% had active nephrotic syndrome and received RTX with the purpose of inducing remission. In addition, 71% of patients had previously received one or more immunosuppressive therapies, whereas 29% were receiving a non-steroid immunosuppressive treatment for the first time. This reflects a change in how RTX has been used over time, with some recently diagnosed patients receiving it as their first-line immunosuppressive agent.
The distinction between MCD and FSGS, now believed to represent a continuum of the INS disease, was indeed interesting. In our cohort, we did not observe any difference regarding MCD vs FSGS patients in regard to the risk of relapse following RTX, but there was a non-significant trend linked to the steroid-responsiveness. In our opinion, this supports that resistance to treatment (particularly steroids) might be a more valuable criterion than histology at the time of diagnosis when assessing the severity of INS in adult patients.
AJKD Blog: Your primary endpoint was a relapse of disease following the first RTX dose for patients in partial or complete remission, and a secondary endpoint of safety looking at infectious episodes. Your paper mentions the definitions of these were based on the most recent KDIGO guidelines, but can you remind our readers what the definitions of complete and partial remission are, and how relapses were defined?
AUTHORS: The KDIGO guidelines define complete remission as proteinuria <300 mg/g with a serum albumin>3.5 g/dL. Partial remission is defined as proteinuria between 300 and 3,500 mg/g together with a reduction of more than 50% from baseline.
A relapse is defined as proteinuria >3,500 mg/g after complete remission, or an increase in proteinuria of more than 50% in patients who were previously in partial remission.
In our study, we chose to base our definitions on these recommendations, with a few practical adaptations. We defined complete remission as proteinuria <300 mg/g and partial remission as proteinuria between 300 and 3,500 mg/g. Relapse was defined as the recurrence of nephrotic syndrome in patients who had achieved complete remission, or as a doubling of proteinuria in patients who were in partial remission.
We considered serum albumin only when defining nephrotic syndrome, which we defined as a protein–creatinine ratio >3,500 mg/g together with an albumin level <3 g/dL. In practice, serum albumin can be difficult to interpret, particularly in retrospective studies. While proteinuria provides a relatively immediate measure of disease activity, albumin levels often take longer to normalize and can be influenced by several other factors which complicate its interpretation.
AJKD Blog: Moving on now to the results, it looks like the median age for the first RTX dose was around 36, and about two-thirds of patients had already received steroids or another immunosuppressive drug before this. What were the main findings when looking at the relapse rates of these patients who received RTX?
AUTHORS: In our cohort, age was not significantly associated with the risk of relapse. However, receiving one or more immunosuppressive treatments at the time of the first RTX infusion was significantly associated with a higher risk of relapse over time. This likely reflects differences in disease severity. Patients who required multiple immunosuppressive therapies before or at the time of RTX probably had more difficult-to-control INS, which may explain the lower durability of remission observed after the first rituximab infusion.
AJKD Blog: One of the challenges in interpreting these data is that your cohort includes patients who are in remission and doing quite well, but also others who were refractory to initial therapy. What did you find with regards to the use of RTX in patients who either had frequent relapses or never attained any form of remission?
AUTHORS: 26 of the 134 patients were not in remission at the time of the first RTX infusion, and were classified as refractory. In these cases, RTX was introduced despite ongoing nephrotic syndrome which may reflect two different scenarios. In some patients, clinicians may choose to introduce RTX early in the course of a complicated nephrotic syndrome, with the goal of achieving remission more rapidly rather than waiting for the full effect of corticosteroids. In other cases, it reflects disease that remains difficult to control, with persistent nephrotic syndrome despite corticosteroids and several prior immunosuppressive therapies.
Interestingly, these refractory patients still showed a meaningful response to RTX. Among the 26 patients, 19% achieved complete remission and 46% achieved partial remission within six months of the first infusion. However, we did observe differences between responders and non-responders. Among patients who responded to RTX, there was a significantly higher proportion of patients with MCD, as well as a higher proportion of patients who had not previously received immunosuppressive treatments other than corticosteroids.
AJKD Blog: Was RTX used beyond the initial dose as maintenance in patients in your study? What did you find with regards to patients who got an additional dose at 6 months?
AUTHORS: During data collection, we noticed that many clinicians were already using maintenance doses of RTX to sustain remission, in a strategy somewhat similar to what is done in ANCA-associated vasculitis. This practice had developed despite the lack of robust evidence at the time. When we looked at the raw data, we had the impression that this approach might be effective, and we wanted to formally evaluate it.
In our cohort, 61 of the 134 patients received one or more maintenance courses of RTX during follow-up. Among the 102 patients who were in complete or partial remission six months after the first course, 22 received a reinjection at six months. This additional dose was associated with better relapse-free survival at 24 months (89.6% vs 66.3%).
Because patients did not systematically receive a reinjection at six months, we also built a marginal structural model to more robustly assess the effect of maintenance therapy, focusing on reinjections administered between 6 and 12 months. In this model, RTX reinjection during this period was significantly associated with a reduction in long-term relapse risk, with a hazard ratio of 0.35.
AJKD Blog: RTX is often touted as a “steroid-sparing” agent. What were the overall effects of these patients receiving RTX when looking at their steroid dosing?
AUTHORS: We observed a clear steroid-sparing effect of RTX in our cohort. Among the 104 steroid-sensitive patients, the proportion receiving corticosteroids decreased significantly as early as six months after rituximab, dropping from 89% at baseline to 39% at month 6. This reduction was sustained over time. By 24 months, only 19.7% of patients were still receiving corticosteroids. In addition, among those who remained on steroids, the daily dose was substantially lower, with a mean dose of 10 mg/day at month 6, compared with 43 mg/day at baseline. We also observed a significant reduction in the use of other immunosuppressive therapies. At the time of the first RTX infusion, 41% of patients were receiving another immunosuppressive agent in addition to corticosteroids. This proportion decreased to 13% at months 6 and 24.
AJKD Blog: Your secondary endpoint was looking at the safety of this drug. Were there any signals that RTX increased the risk of infections for either the initial or those who received follow-up maintenance?
AUTHORS: We did not observe an increased risk of severe infections (requiring hospitalization) in patients receiving rituximab as maintenance therapy. However, these findings should be interpreted with caution, as our cohort was retrospective. Patients selected for maintenance RTX were likely chosen by their nephrologists based on a perceived low infectious risk. Regarding infections after the initial infusion, we did not include a control group treated with corticosteroids or CNIs. Therefore, our study cannot draw conclusions about the relative infectious risk of RTX compared with other immunosuppressive therapies. It should be noted that two patients in our cohort died from infectious causes. Although this is one of the largest adult rituximab cohorts available, only 134 patients were included and the study was retrospective. Therefore, we recommend continued vigilance and careful assessment of the benefit-risk balance, particularly in older or frail patients, when considering B-cell–depleting therapy.
AJKD Blog: Final question is what are your major takeaways from the paper, and can you provide any insight into ongoing studies in the field of RTX use for nephrotic syndromes that will hopefully give us more information in the future?
AUTHORS: RTX appears to be an effective therapy for reducing exposure to corticosteroids and other immunosuppressive agents, and it clearly has a place in the treatment strategy for adult INS. Importantly, RTX also shows meaningful efficacy in refractory patients, with more than half achieving partial or complete remission within six months, particularly in patients with MCD or those with a recent diagnosis without prior immunosuppressive exposure.
In adults, RTX significantly reduces the risk of relapse and helps maintain long-term remission. This supports using the drug earlier in the treatment course, as reducing relapses also limits re-exposure to corticosteroids and other immunosuppressants, potentially decreasing side effects such as hypertension, diabetes, and infections. We are particularly looking forward to the results of the RIFIREINS trial, an ongoing prospective French study evaluating RTX in the first episode of adult MCD. While our data, along with many observational studies, suggest that RTX is effective for first episodes or relapses of INS, prospective randomized studies are needed to confirm these findings. In this context, the ongoing TURING trial, a randomized controlled study assessing RTX in newly diagnosed or relapsing INS, will hopefully provide definitive evidence to guide clinical practice.
To view Laslandes et al [subscription required], please visit AJKD.org:
Title: Response to Rituximab as a Maintenance Therapy in Adult Idiopathic Nephrotic Syndrome: A French Multicenter Cohort Study
Authors: Manuel Laslandes, Marine Lorent, Benoit Brilland, Hugoline Boulay, Léonard Golbin, Christelle Barbet, Jimmy Grellier, Amaury Dujardin, David Larmet, Angelo Testa, Pierre Pfirmann, Antoine Thierry, Simon Ville, Jacques Dantal, Christophe Masset
DOI: 10.1053/j.ajkd.2025.09.021
Leave a Reply