
Re-centering Primary Care in the Long-Term Care of Living Kidney Donors
Dr. Justin Oveyssi is an Assistant Clinical Professor of Medicine in Transplant Nephrology at UCSF. His clinical and academic work focuses on post–kidney transplant care, including immune-mediated complications and long-term outcomes in transplant recipients. He is passionate about improving care coordination and long-term follow-up for living kidney donors and transplant patients.

Living kidney donors are often described as heroes. They are individuals who voluntarily accept surgical and medical risks so that someone else may live a longer and healthier life. However, after the surgery is complete and transplant clinic visits end, a fundamental question remains: who is responsible for the long-term care of the living kidney donor?
Wong-Mersereau and colleagues performed a qualitative study that presents a perspective that is not often highlighted in transplant nephrology: that of family physicians who care for patients after living kidney donation. What emerged was not a lack of willingness to provide care, but rather a lack of clarity and infrastructure in how to provide adequate and necessary care post-donation. Kidney donors are not common patients in most primary care practices. Many primary care providers (PCPs) encounter only a handful of such patients over the course of their careers. In an era when primary care clinics are overloaded and competing priorities are constant, dedicating continuing education time to a patient population encountered so infrequently can be difficult to justify. Yet from the perspective of transplant nephrology, high-quality donor follow-up is essential for early detection of healthcare risks and for long-term outcome data that informs future selection of kidney donors.
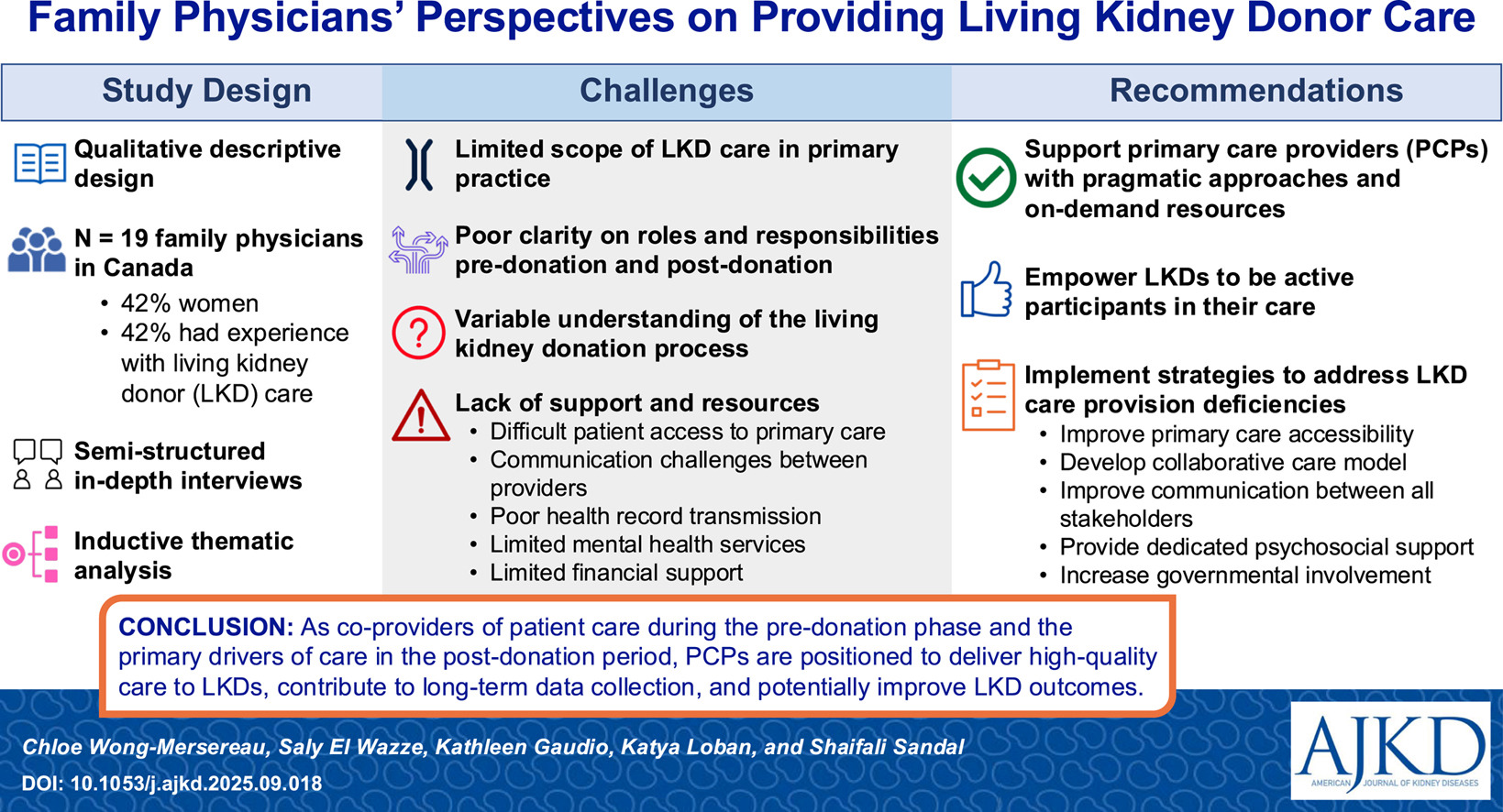
The study revealed that even before donation occurs, primary care physicians sometimes express apprehension about participating in preoperative risk counseling. Despite this, they remain willing partners in helping patients navigate questions, healthcare systems, and next steps. Following donation, living donors face increased risks of hypertension, reduced kidney function, and complications during pregnancy, albeit the absolute risks remain low. Transplant teams emphasize the importance of lifelong monitoring of blood pressure, serum creatinine, and albuminuria. Herein lies the paradox: what is considered essential within transplant nephrology is often less visible within the broader landscape of primary care. After donation, many PCPs reported that they feel comfortable managing chronic disease, screening for depression, monitoring laboratory results, and coordinating referrals if expectations and responsibilities are clearly defined. The issue, therefore, is not commitment, but structure.
Participants described fragmented communication with transplant programs, difficulty accessing transplant records, limited psychosocial resources, and a substantial volume of uncompensated administrative tasks. These are not minor inconveniences. Rather, they represent systemic shortcomings that gradually erode effective long-term follow-up.
Follow-up has been shown to be inconsistent, even within universal healthcare systems. Data from this study suggest that only about one-quarter of kidney donors receive the recommended annual monitoring markers over approximately seven years. Because transplant programs often cannot sustain indefinite follow-up internally and primary care lacks standardized tools for donor monitoring, donors may drift into a gray zone of shared but diffuse responsibility.
Encouragingly, the study also suggests practical solutions. Family physicians are primarily asking for clarity and efficiency:
- A concise, jurisdiction-specific guide outlining donor pathways
- Clear delineation of pre- and post-donation responsibilities
- EMR-integrated reminders or templates
- Direct communication pathways to transplant programs
- Structured psychosocial resources
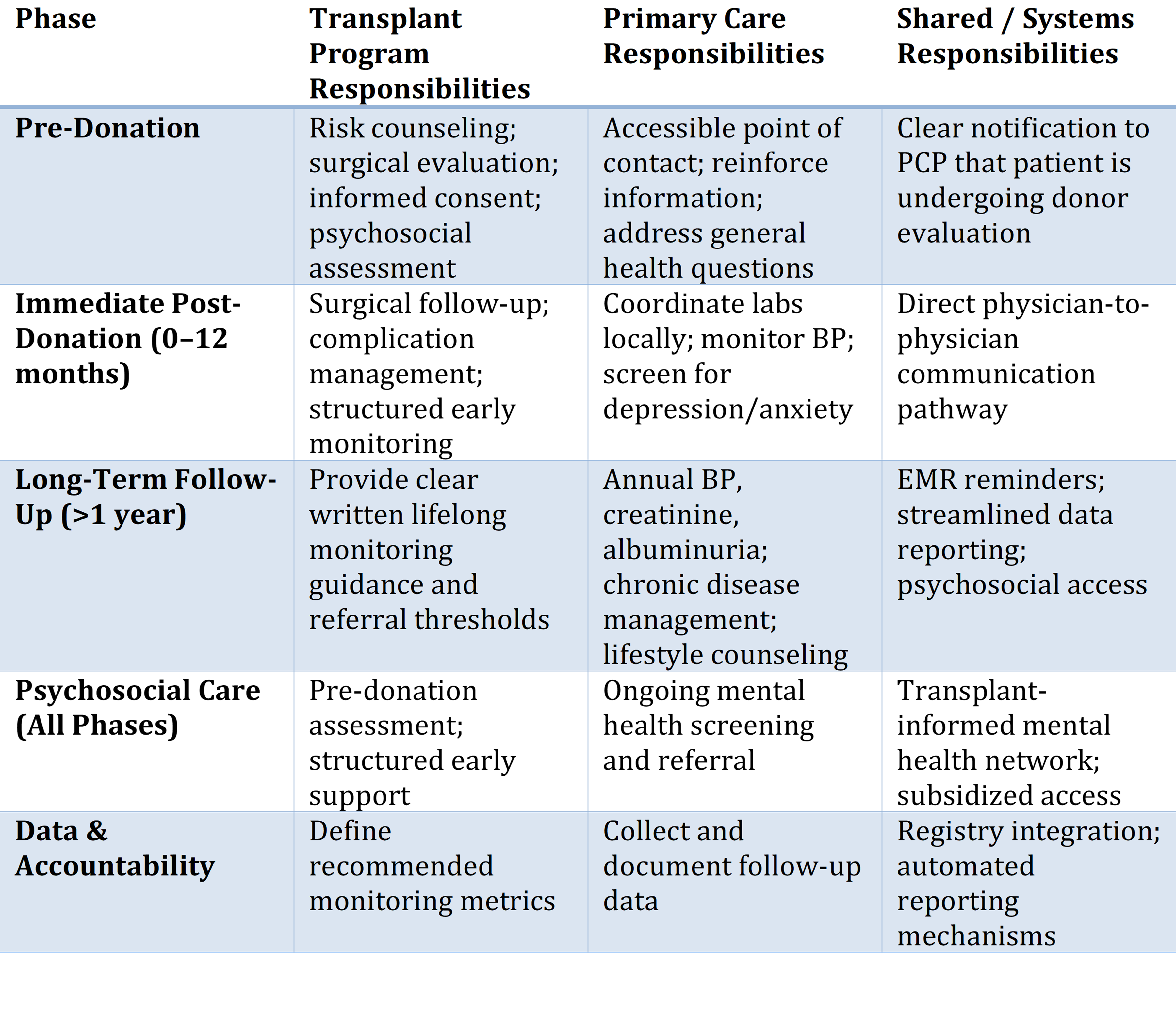
Below is a simplified shared-care model that translates the study’s themes into an operational framework:
Table 1. Proposed Shared-Care Model for Living Kidney Donor Follow-Up
 Perhaps one of the most striking insights from this study is the importance of empowering kidney donors themselves. While turnover in primary care and educational gaps are common, an informed donor may represent the most stable element of long-term care after donation. When donors understand which laboratory tests are needed annually, what blood pressure targets matter, and when to reconnect with transplant teams, they become active partners rather than passive recipients of follow-up care.
Perhaps one of the most striking insights from this study is the importance of empowering kidney donors themselves. While turnover in primary care and educational gaps are common, an informed donor may represent the most stable element of long-term care after donation. When donors understand which laboratory tests are needed annually, what blood pressure targets matter, and when to reconnect with transplant teams, they become active partners rather than passive recipients of follow-up care.
The number of living kidney donors continues to grow globally. With this growth comes a rising number of donors with higher baseline medical risk. This reality requires not only transparent disclosure of risk at the time of donation but also credible, durable pathways for long-term care.
Donors must be able to trust that they will not be forgotten if their health changes years later. This study reminds us that primary care physicians are not barriers; rather, they are essential partners in the care and follow-up of living donors. For primary care physicians to succeed in this role, they require clarity, infrastructure, and collaboration. The question is whether we will design that partnership intentionally or allow it to remain fragmented and disorganized. If we truly wish to honor those who have given a kidney so that someone else may live, the answer should be intentional.
-Post prepared by Justin Oveyssi
To view Wong-Mersereau et al [Subscription required], please visit AJKD.org:
Title: Family Physicians’ Perspectives on Providing Living Kidney Donor Care
Authors: Chloe Wong-Mersereau, Saly El Wazze, Kathleen Gaudio, Katya Loban, and Shaifali Sandal
DOI: 10.1053/j.ajkd.2025.09.018
Leave a Reply