
NephMadness 2016: International Nephrology Region

Submit your picks! | For more on NephMadness 2016 | #NephMadness or #WorldNephRegion on Twitter
NephMadness and all of social media break down traditional geographic barriers. When we tweet, we tweet to the world. Our nephrology social media community has members from every corner of the globe. As our world shrinks, what happens in previously remote areas can walk into your clinic as the next patient. The International region highlights four issues that are shaking nephrology. At the top of the bracket are two mysterious epidemics, one an epidemic of AKI due to traditional herbal remedies and the other an epidemic of CKD mainly affecting young male agricultural workers in tropical climates. In the bottom half of the bracket we have the exotic world of international transplant. Each country’s ethnic and cultural background affects its approach to transplant. This provides a rich variety of transplant behaviors from which we can learn to craft a better experience for our patients. Rounding out the region is the the league’s bad boy: transplant tourism. A crafty side effect of capitalism, transplant tourism turns the kidney into just another valued commodity. Transplant tourism exploits the vulnerable and entices them to put their health at risk by selling organs. This is an important issue and nephrologists should have a voice in policies designed to curb this behavior.
Selection Committee member for the International Nephrology Region:
Professor Vivekanand Jha, MD, DM, FRCP
Prof Jha is a Professor of Nephrology at the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He is the councillor of the International Society of Nephrology and the Chair of ISN Education. He has been involved in several KDIGO clinical practice guidelines and controversies conferences. Among others, he is interested in investigating the global diversities of kidney disease and its determinants.
Meet the Competitors for the International Nephrology Region
Traditional Remedies and Kidney Failure
CKDu (Mesoamerican) Nephropathy
Transplant Tourism
Organ Procurement
Traditional Remedies and Kidney Failure vs CKDu (Mesoamerican) Nephropathy
Traditional Remedies and Acute Kidney Failure
 Traditional (or herbal) Remedies has been playing for longer than anybody from the pharmaceutical conferences, but they have just recently been getting invited to the tournament. Aristolochia made an appearance in NephMadness in 2014 and won the Toxin Region, but fell to eventual NephMadness Champion, JNC8. This year, we see the return of Traditional Remedies in a first round match-up against CKDu. Traditional Remedies are widely used in both the developing and developed world. A 1997 survey showed that one in nine adults used herbals, to the tune of $5.1 billion. An Australian survey—found that one in four adults used traditional remedies. In Africa, China, and India, these numbers swell to 65-80%. In many countries traditional medicine is not alternative at all, but is recognized and supported by central and provincial governments. Traditional Chinese and Indian Ayurvedic and Unani medicines are examples of this.
Traditional (or herbal) Remedies has been playing for longer than anybody from the pharmaceutical conferences, but they have just recently been getting invited to the tournament. Aristolochia made an appearance in NephMadness in 2014 and won the Toxin Region, but fell to eventual NephMadness Champion, JNC8. This year, we see the return of Traditional Remedies in a first round match-up against CKDu. Traditional Remedies are widely used in both the developing and developed world. A 1997 survey showed that one in nine adults used herbals, to the tune of $5.1 billion. An Australian survey—found that one in four adults used traditional remedies. In Africa, China, and India, these numbers swell to 65-80%. In many countries traditional medicine is not alternative at all, but is recognized and supported by central and provincial governments. Traditional Chinese and Indian Ayurvedic and Unani medicines are examples of this.
The primary source of danger from traditional medicines is not that they may be merely expensive placebos, but rather many of them have potent biochemical effects but there is little known about the pharmacology of the compounds as they are used in practice. The problem can start with something as banal as nomenclature. This was at the root of the aristolochia disaster where toxic guang fang ji (Aristolochia fangchi) was substituted for the benign han fang ji (Stephania tetrandra) leading to an epidemic of ESRD among previously healthy, middle-aged, women. If you are not familiar with this story make sure to read about Aristolochic acid nephropathy or Chinese Herb Nephropathy. Nomenclature is just the start of the problem. A medication’s recipe is often folklore and passed from generation to generation as an oral tradition. Secrecy surrounding specific ingredients makes pharmacologic analysis essentially hopeless.
Traditional remedies can have systemic toxicity but the kidneys are a particularly ripe target:
- Kidneys receive 20-25% of the cardiac output, so there is a lot of exposure
- Large endothelial surface area
- High metabolic activity
- Active uptake and concentration of toxins in the tubules
- Hypoxia, in the thin limbs of the loop of Henle, increases tissue susceptibility
- Acidotic urine can activate toxins
The primary cause of acute kidney injury with traditional remedies is acute interstitial nephritis (AIN). ATN and pre-renal azotemia are the other major causes of AKI with traditional medicines.
Other abnormalities include:
- Hypokalemia from licorice, a common additive to traditional Chinese medicine to make them more palatable
- Hyperkalemia from alfalfa or noni juice
- Hematuria from anticoagulant properties of Ginko biloba
St John’s Wort induces P450 and MDRP1 to lower the bioavailability of many medications including the calcineurin inhibitors. Cases of acute kidney rejection from St John’s wort are particularly upsetting.
The outcomes depend on the medical setting. Rural Africa has few resources available to patients with advanced CKD. Mortality in these regions can vary from 25% to 60%. In the West, access to renal replacement therapy lowers mortality but still represents a devastating illness for the patient who may continue to ingest “safe natural supplements” without knowledge of the physician.
Examples
- Callilepis laureola poisoning – Popular in Sub-Saharan Africa, including South Africa. Widely used for numerous indications including: bad dreams, fertility, decongestant, sexually transmitted disease, or to ward off evil spirits. Half the population of Natal consumes Callilepis laureola and it is the most common cause of AKI in Africa. Renal failure is seen in 60% of patients with drug toxicity and mortality is 50%.
- Djenkol bean poisoning – This is widely consumed in South East Asia. In adequate doses it can lead to djenkolism – A symptom complex of dysuria, lumbar pain, hypertension, hematuria and oliguria. Djenkolic acid forms needle-like crystals that precipitate and cause tubular obstruction. Precipitation is induced by high concentrations and low pH.
- Propolis – it is a resinous substance collected by honeybees and claimed to have antiseptic, astringent, and anti-inflammatory properties. Most of its use and toxicity has been reported from South America and is a cause of oliguric AKI.
The problem of kidney injury due to herbal or alternative medications is huge, under reported, and global. By better understanding the mechanisms of how these agents contribute to kidney damage could aid in developing novel therapies.
CKDu (Chronic Kidney Disease of Unknown Etiology) or MAN (MesoAmerican Nephropathy)
 CKDu or Mesoamerican nephropathy is more of an admission of defeat than a specific disease entity. In the 1990s, increased end-stage renal disease and demand for dialysis emerged in both El Salvador and Sri Lanka. These cases of ESRD did not follow the epidemiologically common causes of ESRD, e.g., the patients were younger and largely free of diabetes and hypertension. These unusual cases of CKD and ESRD began to be recognized in other countries including Nicaragua, Guatemala, Honduras, India, and Egypt. As these diseases were recognized, they were often given regional names: Central American nephropathy, Salvadoran agricultural nephropathy, Mesoamerican epidemic nephropathy, chronic tubulointerstitial kidney disease of Central America, Udhanam endemic nephropathy (India), and Sri Lankan agricultural nephropathy. To better track this, all of these regional epidemics are lumped together as CKD of unknown etiology or CKDu or CKD due to non traditional causes (CKDnt). CKDu is a phenotypic description rather than a pathological entity and possibly due to more than one etiological factor. Necessarily it is a diagnosis of exclusion. While there is no internationally accepted case definition, common characteristics across studies include the following:
CKDu or Mesoamerican nephropathy is more of an admission of defeat than a specific disease entity. In the 1990s, increased end-stage renal disease and demand for dialysis emerged in both El Salvador and Sri Lanka. These cases of ESRD did not follow the epidemiologically common causes of ESRD, e.g., the patients were younger and largely free of diabetes and hypertension. These unusual cases of CKD and ESRD began to be recognized in other countries including Nicaragua, Guatemala, Honduras, India, and Egypt. As these diseases were recognized, they were often given regional names: Central American nephropathy, Salvadoran agricultural nephropathy, Mesoamerican epidemic nephropathy, chronic tubulointerstitial kidney disease of Central America, Udhanam endemic nephropathy (India), and Sri Lankan agricultural nephropathy. To better track this, all of these regional epidemics are lumped together as CKD of unknown etiology or CKDu or CKD due to non traditional causes (CKDnt). CKDu is a phenotypic description rather than a pathological entity and possibly due to more than one etiological factor. Necessarily it is a diagnosis of exclusion. While there is no internationally accepted case definition, common characteristics across studies include the following:
- Asymptomatic and progressive CKD as defined by international standards
- Absent or sub-nephrotic proteinuria
- Absence of hematuria
- Absence of diabetes, chronic or severe arterial hypertension, HIV, snake bite, glomerulonephritis, or other urinary tract disease
- Normal glycosylated hemoglobin (<6.5%)
- Normal(ish) blood pressure
- <160/100 mmHg in untreated patients
- <140/90 mmHg in patients receiving up to 2 antihypertensive drugs
This new entity is burning up the actuarial charts moving CKD into the fifth most common cause of death in Central and Andean Latin America. Mortality from CKD increased 350% in the last 20 years and the second most common cause of CKD in India. (Lozano R et al, Lancet 2012, Global Burden of Disease, Martin-Cleary et al, Clin Kidney J, 2014, Rajapurkar et al BMC Nephrol 2012).
Despite the various names and the wide foot print of the disease, some characteristics seem to be consistent from region to region. This disease affects more men than women and it tends to strike at a younger age (mean age 35 years), often in the prime of life. Agricultural workers are the hardest hit. El Salvador and Nicaragua have the highest prevalence of CKDu, up to 16% of the population (compare with ~5% in North America and Europe). In El Salvador ESRD due to CKDu is now the leading cause of hospital mortality and El Salvador can now claim the highest mortality rate from CKD in the world at 51.8 deaths per 100,000.
The risk factors for CKDu were explored by a systematic review of 26 articles from Central America and South Asia. Most data were cross sectional or case-control data of variable quality. The top risk factors in South Asia are exposure to heavy metals, farming, family history, agrochemical use and smoking. The risks in Central America were age, male sex, agrochemical use, farming and heat stress. This re-emphasizes the clinical phenotype of a young male agricultural farmer working long hours in hot humid conditions, but given the variable quality of the studies making up the systematic review caution should be used in relying on the results.
One attractive hypothesis is that the combination of recurrent dehydration, heat stress, and high sugar intake, usually as sugar sweetened beverages, is a primary driver of CKDu. The finding of increased CKDu at lower, hotter altitudes supports this theory. This theory was explored in one of the first NephJCs. Laws et al recently published their study results in AJKD where they identified high IL18 and NGAL levels in Nicaraguan sugarcane workers involved in heavy field labour, though this may be just one side of a complex matrix.
While several researchers continue to explore this baffling entity there remain several unanswered questions.
- Is CKDu a truly global disease?
- Is it the same entity with similar pathophysiology everywhere?
- When did it begin in these countries?
- Are there countries where it exists but has not yet been detected?
Thus, what we have on our hands is a global phenomenon of unexplained CKD which is cutting down young, productive, men in prime of their life. Most of these young men are dying without hope. The epidemic demands urgent answers.
Transplant Tourism OR Organ Trafficking vs Organ Procurement
Transplant Tourism OR Organ Trafficking
 Organ transplant tourism is similar to the illicit drug trade. There is money, desperation, crime, organized syndicates, black market, people trafficking including children. All countries actively pursuing transplantation have some form of educational program to improve the awareness of organ donations—both living and deceased. However, the Global Observatory on Donation and Transplantation (GODT) Report reveals that despite 118,127 transplants in 2014 this met less than 10% of the global demand for organs. This makes the situation ripe for crime, only this time the commodity is human organs. It is time we reconcile that the beautiful experience of organ donation has such an ugly side.
Organ transplant tourism is similar to the illicit drug trade. There is money, desperation, crime, organized syndicates, black market, people trafficking including children. All countries actively pursuing transplantation have some form of educational program to improve the awareness of organ donations—both living and deceased. However, the Global Observatory on Donation and Transplantation (GODT) Report reveals that despite 118,127 transplants in 2014 this met less than 10% of the global demand for organs. This makes the situation ripe for crime, only this time the commodity is human organs. It is time we reconcile that the beautiful experience of organ donation has such an ugly side.
Transplant tourism has been around for a long time and Trafficking in Humans for Organ Removal (UN Assessment ToolKit) was recognized two decades ago. The world’s poorest, illiterate, prisoners, undocumented immigrants, political or economic refugees are providing organs for the wealthy (Bagheri, 2015). Adding to the misery is the newer trend of trafficking humans themselves to serve as organ donors. To add to this disturbing picture are the reports of murdered children whose bodies turn up minus their organs (Secretary General Report UN 2006).
The plight of the donors after the transplant is pretty terrible, among the problems these donors have:
- They have no way to get medical follow up
- They receive a tiny portion of the price of the organ as most of the money is sucked up by slick “facilitators” leaving a pittance in the hands of the donor. The donors are often in debt but after paying off the loan, the donor often returns to debt within years of the donation.
- These situations have driven some donors to suicide
A survey of 239 kidney “vendors” from Pakistan presented very disturbing statistics. These commercial donors were 34 years old, 90% illiterate, 69% bonded laborers with monthly income of $16 US. Ninety percent underwent “donation” for debt repayment of ~$1300 and were paid a mean of ~$1400. However, on follow up 88% identified no improvement in their financial status and 98% reported deterioration of their own health.
Organ trafficking is a global phenomenon. Among the countries with confirmed reports are Egypt, Pakistan, Sudan, India, China, Philippines, and Mexico. In a recent report, the Daily Mail identified an even more disturbing trend of terrorist organisations recruiting foreign doctors to help harvest organs not only from their dead comrades but also from living hostages from Syria and Iraq. Transplant tourism in China takes an even more disturbing turn where death row prisoners are a significant source of organs for transplant.
Organ trafficking has been defined after the Istanbul Declaration (2008) as:
‘‘The recruitment, transport, transfer, harboring, or receipt of living or deceased persons or their organs by means of the threat or use of force or other forms of coercion, of abduction, of fraud, of deception, of the abuse of power or of a position of vulnerability, or of the giving to, or the receiving by, a third party of payments or benefits to achieve the transfer of control over the potential donor, for the purpose of exploitation by the removal of organs for transplantation.”
Transplant Tourism has become a synonym for organ trafficking and is defined by UNOS as ‘the purchase of a transplant organ abroad that includes access to an organ while bypassing laws, rules, or processes of any or all countries involved’. It accounts for 5-10% of all kidney transplant worldwide but this data is very difficult to come by and possibly an underestimate.
The following cartoon shows various models of transplant tourism. This concept was presented by Yosuke Shimazono at the Second Global Consultation on Human Transplantation at the WHO headquarters in Geneva in 2007:

Mode 1

Mode 2
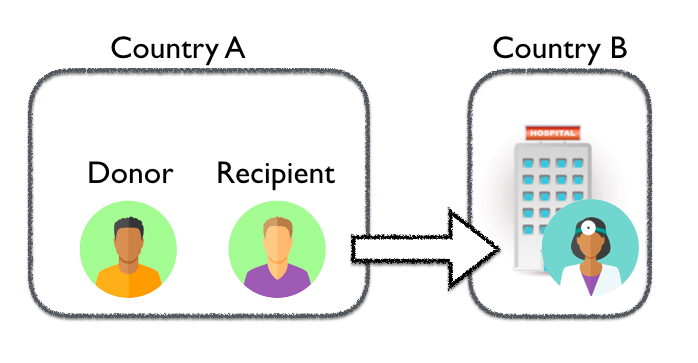
Mode 3

Mode 4
Data from certain countries is startling (most of this data is not published in any registry unsurprisingly, but derived from interviews and visits). In Pakistan 2,000 kidney transplants were performed for foreign tourists, the donor source however is uncertain. In Philippines there are reports of more than 3,000 transplants for foreigners, with certain districts encouraging transplant tourists. In India, there are increasing reports of organ transplants to foreigners with the organ source often being the tsunami victims from Chennai. Egypt performs about 500 transplants from commercial donors. Several hundred ESRD patients from countries like Saudi Arabia, Taiwan, Malaysia, and South Korea went abroad for a transplant according to data compiled by Shimazono et al and presented at the Second Global Consultation at UN. The largest number of transplants is from China where 11,000 transplants were conducted from executed prisoners of which 8,000 were kidney transplants. Since then several measures were taken by Chinese authorities to curb this menace and it was declared last year that this practice has been stopped, as presented by Dr Delmonico at the WCN 2015. However, there are still doubts.
When a patient asks about buying a kidney or tells you of her plans to get a foreign commercial kidney what is your role? Timothy Caulfield from the University of Alberta explores the legal and ethical issues surrounding this question. Physicians and other healthcare providers in the field of ESRD are well placed to play a role in monitoring and reducing these practices. Oftentimes the patient will ask this question before leaving and these are opportunities to dissuade the recipient.
- Physicians should provide information about the ethical issues surrounding this practice—Click here for an excellent pamphlet in several languages to provide the patients with information.
- Provide an honest assessment of health risks involved
- Description of possible complications and the lack of continuity in care needs to be outlined
- The plight of the organ donor needs to be conveyed to the potential “tourist”
These discussions may invoke a person’s conscience and ethical integrity and hopefully prevent this sometimes fraudulent activity. Picolli et al explores this question of “Doctor can I buy a kidney” from an ethical lens and helps physicians apply a concept of “reverse” informed consent (where the patient asks advice) using four ethical principles: beneficence, non-maleficence, justice, and autonomy.
Can a physician disclose that his/her patient bought a kidney? In most states there is no obligation to do this and it can have a negative impact on the patient/physician relationship so information should be provided before the transplant.
Organ Procurement
 Worldwide, CKD is increasing. Every year the number of patients starting dialysis and being waitlisted for a transplant goes up. Also increasing is the number of people dying without ever getting a transplant.Globally, CKD has among the highest percent increase in deaths over the last two decades.
Worldwide, CKD is increasing. Every year the number of patients starting dialysis and being waitlisted for a transplant goes up. Also increasing is the number of people dying without ever getting a transplant.Globally, CKD has among the highest percent increase in deaths over the last two decades.

Data from the Global Burden of Disease website
Tragically, donor pools cannot keep up with increased demand so a smaller fraction of waitlisted patients are being transplanted every year. Over the years most countries have developed organ procurement policies and organizations to facilitate the organ donation. In United States the UNOS/OPTN work side-by-side with the transplant centers to match donors and recipients across the nation. In Canada, the Canadian Blood Services and Canadian Transplant Registry work with provincial partners to do the same. EuroTransplant is the organ procurement organization for seven European nations. The United Kingdom and Spain have their own corresponding systems. China and India’s ESRD populations are immense but cultural and religious beliefs coupled with poverty and illiteracy have kept the rates of both living and deceased organ donation below levels seen in western countries. Living related donation continues to be altruistic in most part but the living unrelated donation is speculated to be have a commercial angle to it especially in the poor countries.
Organ procurement from deceased donor follows two broad principles.
- OPT-OUT (Presumed Consent): Meaning every individual is considered for organ donation on death unless specifically mentioned as not willing to donate. Thus, the DEFAULT is to be a donor
- OPT-IN (Explicit Consent): When the person has to have made his wish of donating organs after his/her death known and have a donor card signed. Thus, the DEFAULT is not to be a donor
Countries with OPT-OUT or Presumed Consent
Argentina, Austria, Belarus, Belgium, Bulgaria, Colombia, Costa Rica, Croatia, Czech Republic, Ecuador, Finland, France, Greece, Hungary, Italy, Latvia, Panama, Poland, Portugal, Russia, Singapore, Slovak Republic, Spain, Sweden, Tunisia
Countries with OPT-IN or Explicit Consent
Australia, Brazil, Canada, Cuba, Denmark, Germany, Guatemala, Hong Kong, Republic of Ireland, Israel, Japan, Lebanon, Lithuania, Malaysia, Mexico, The Netherlands, New Zealand, Puerto Rico, Romania, Taiwan, UK, USA, Venezuela
In a study comparing these policies and effect on transplant rates in 44 transplanting countries, Horvat LD et al, showed that having presumed consent policy in the country pushed up the rates of deceased donor transplant but these countries had lower living donor transplant rates. Thus, it a fine line to walk—adopting presumed consent as a policy may adversely affect living donor rates:
- Deceased donor kidney transplantation rates
- OPT-OUT – countries (n=22): 22.6 transplants per million
- OPT-IN -countries (n=22): 13.9 transplants per million
- Living donor kidney transplantation rates
- OPT-OUT countries 2.4 transplants per million
- OPT-IN countries 5.9 transplants per million
These data were confirmed by Shepherd et al showing deceased donor transplants were higher in the OPT-OUT countries at the cost of the living donation. Despite this unfortunate consequence, the total number of kidneys and livers transplanted were still higher in OPT-OUT countries.
Rosenbaum et al studied the role next-of-kin play in deceased organ donation. In 54 nations with both presumed or explicit consent most physicians do not proceed without the next-of-kin OK. This important to incorporate into education regarding donation. It should have a next-of-kin message to improve organ procurement.
Spanish Model of Organ Donation—Why are the spaniards so asombros. Spain has the world’s highest rate of organ donation, short waiting lists, and reduced reliance on living donation. Highlights of the Spanish model include
- OPT-OUT since 1979
- Highest proportion of ICU beds in the world
- Universal healthcare including transplant
- Extensive training of doctors with every aspect of donation counselling
- Each hospital has its own transplant coordinators
- Unlike other countries these transplant coordinators are the same healthcare professionals working in the ICU who work part-time as Tx coordinators
Country-wise specifics of organ procurement (Jingwei AH et al, 2010):
- China – 90% of deceased organ transplant occur from executed prisioners. In 2015 the Chinese authorities made an announcement to end the practice; however, the clause that prisoners still have full rights in terms of organ donations and can therefore “voluntarily” donate organs after they are executed still remains, casting a doubt on the real effect of the announcement.
- India – By law the living donor organ transplants can occur between first degree relatives only; this was recently expanded to include grandparents and grandchildren. Anyone beyond this degree of relation is considered a Living Unrelated Donor and undergoes several assessments by a committee to identify and stifle the commercialization of organs.
- Taiwan – Has a rapidly aging population and decreased availability of organs, despite having a broad definition of living related transplant. By National Health Insurance Bureau data, close to half of the patients are transplanted overseas.
- Iran – The Organ Transplantation Act passed in 2000 made the sale of living unrelated kidney donors legal. These commercial donors get anywhere from $2,000-$4,000 for their organ and a supplemental compensation of $1550 from the recipient (Broumand B, Transplantation Activities in Iran, Transplantation Proceedings, 2005). This practice has increased the number of living donations at the expense of the deceased donor program.
- Saudi Arabia – There was an increasing organ shortage in Saudi Arabia leading to several patients to travel abroad for a transplant especially to China, Egypt, Pakistan, and the Philippines. In Oct 2007 the Saudi government started awarding $13,300 for an unrelated organ with lifelong medical care for the donor. This has dramatically increased the number of living donors.
- Japan – Living organ donation forms the bulk of Japanese transplantation. Nearly 70% of all transplants in Japan are living donors.
- Islamic Governments in Indonesia and Iran – Do not allow harvesting organs after death so deceased donor programs are nonexistent or stunted.
What about compensating a living donor?
Living donor and organ procurement has always struggled with the concepts of compensation. Ethically this is challenging—The transplant community is essentially “denying” a right to live by banning the establishment of an open organ market. If such an organ market is created, it will change the very fabric of altruistic donation and may offend cultural, religious, and ethical beliefs of many. The DONOR Network data shows that 40% of all transplants are from living donors. The highest living donation transplant rate was in Saudi Arabia (32 procedures per million population) followed by Jordan, Iceland, and Iran.
The divide in demand and supply of organs has spawned an entire industry of transplant tourism with its attending ethical conundrums and criminal activity. The answer to this global problem lies in encouraging organ donation legally and improving the means of organ procurement in a manner which is justifiable and equitable to the population of the region.
– Post written and edited by Drs. Nikhil Shah and Joel Topf.
![]()
Leave a Reply