
PCI-first or Preemptive Dialysis-first Approach in CKD Patients Needing Cardiac Catheterization
The decision about whether to perform percutaneous coronary intervention (PCI) in patients with advanced stages of chronic kidney disease (CKD) is a challenging one. The well-established risk of contrast-induced nephropathy (CIN) and the chance of precipitating dialysis leads to fear and hesitation on the part of patients, families, cardiologists, and even nephrologists. Balanced against this fear is the knowledge that patients with advanced CKD are at much higher risk for cardiovascular events than the general population, so deferring a cardiac intervention in a CKD patient due to fear of dialysis is one that could potentially lead to serious or fatal outcomes for the patient.
In a recent AJKD article, Khattak et al attempt to evaluate the likely impact of three different strategies for handling stable angina in patients with advanced CKD:
- PCI first, followed by initiation of dialysis therapy only if necessary;
- Medical management of coronary disease; or
- Preemptive initiation of dialysis therapy followed by PCI.
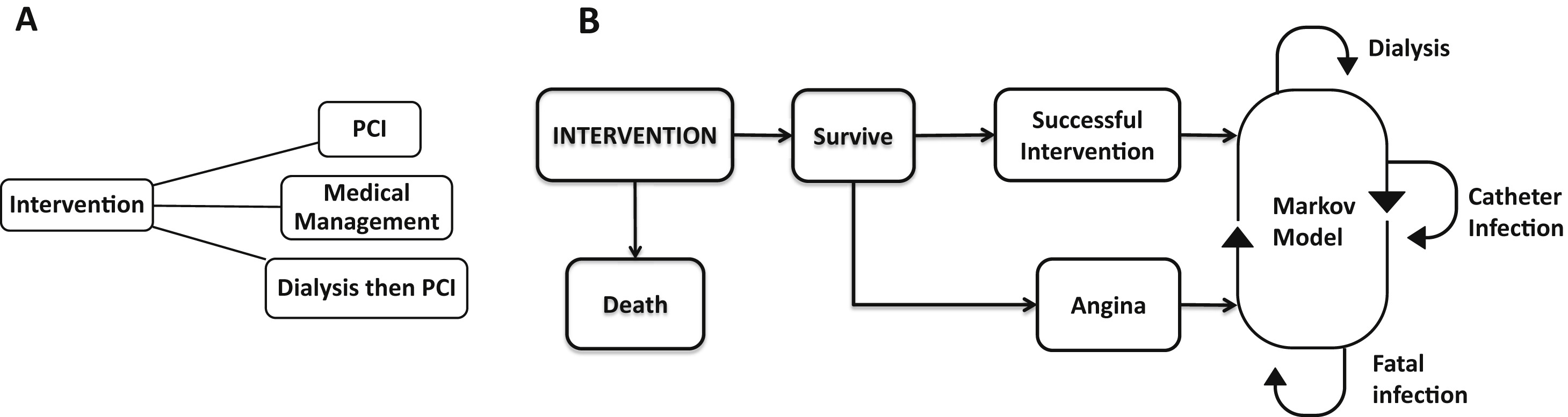
Figure 1 from Khattak et al, AJKD, © National Kidney Foundation. Conceptual model of the decision analysis. (A) Patients are assigned to 1 of 3 treatments as shown in the decision tree. (B) Following an initial treatment choice, participants cycle through the possibilities shown in the Markov model.
The authors used a Monte Carlo simulation and previously published data about expected outcomes, including risks of death on hemodialysis, risks of catheter infection, and anticipated course following medical management or PCI, in order to generate a predictive model for anticipated Quality Adjusted Life Years (QALY) in each of the three strategies.
Khattak et al made several important assumptions about the patient population. The model was designed to evaluate patients with stable angina and factors amenable to a possible PCI (limited disease, discrete areas for intervention). Dialysis initiation was assumed to take place via a tunneled catheter, with patients transitioning to use of a permanent access in 12 months. Data regarding risk of CIN, risks of catheter infection, and risks of death either on or off dialysis were obtained from established literature.
In the simulation model, preemptive initiation of dialysis therapy followed by PCI fared worse than the other two approaches. PCI followed by dialysis only if needed versus medical management were fairly comparable in terms of mean QALY expected (1.103 vs 1.088, respectively; 0.67 for the pre-emptive hemodialysis approach). The authors also made modifications to the simulation to see if these would affect the results. Alternate scenarios included earlier arteriovenous fistula placement or using a lower probability of dialysis dependence following contrast nephropathy, but results were fairly consistent, with the PCI-first approach having a slight advantage, and the preemptive dialysis approach always substantially worse than the other two strategies.

Table 2 from Khattak et al, AJKD, © National Kidney Foundation.
Although it will ultimately take a prospective trial to settle the issue of optimal timing for PCI in patients with advanced CKD, Khattak et al provide very useful information based on expected outcomes in a very well-simulated model. The model predicts no evidence of a reduction in QALY if PCI is undertaken versus medical management. It also does not suggest that PCI in a stable patient improves survival. It may improve symptomatology compared to medical management although that is not proven by this study. Nonetheless, one would hope that a predictive model will help alleviate some of the fear associated with undertaking PCI in this high-risk patient population if medical management is unsatisfactory. Not accounted for by the model is the potential for earlier PCI, reducing the risk of morbidity and mortality after initiation of dialysis therapy, which, if true, would give an advantage to the PCI-first approach.
Post prepared by John W. O’Bell, AJKD Blog Contributor
To view the Khattak et al article abstract or full-text (subscription required), please visit AJKD.org.
Leave a Reply