
#NephMadness 2019: Volume Assessment Region
Submit your picks! | NephMadness 2019 | #NephMadness | #VolumeRegion
Selection Committee Member: Tariq Shafi @DrTariqShafi
Tariq Shafi is a Professor of Medicine, Physiology, and Biophysics, and the John D. Bower Division Director of Nephrology at the University of Mississippi Medical Center. Dr. Shafi’s clinical research focuses on dialysis patients and his active research protocol include studies on cardiac arrhythmias, uremic toxins, resiliency in older adults initiating hemodialysis, and assessment of novel methods for volume management in dialysis patients.
Writer: Devika Nair @devimol
Devika Nair is a nephrology fellow at Vanderbilt University. She served as Chief Nephrology Fellow from 2017-18 and is pursuing a Master of Science in Clinical Investigation during 2017-19. Her research interests involve using qualitative and quantitative methods to study patient-reported outcomes specific to mental health and quality of life among kidney patients as well as finding ways to facilitate better physician-patient communication about these issues.
Competitors for the Volume Assessment Region
Old School vs New School
Dry on Dialysis vs Wet on Dialysis
Copyright: Meryll / Shutterstock
As nephrologists, we are often asked to help evaluate and manage a patient’s volume status. Unlike what is required when identifying florid pulmonary edema or marked volume depletion, our more difficult challenge is often to carefully calibrate volume status according to each patient’s unique physiology. This is no easy task, and there are many instances in which we disagree with our subspecialty colleagues and even with each other on this contentious issue. What is the best way to objectively assess the volume status of patients with end-stage kidney disease (ESKD), and on what volume-related endpoints should we base our fluid management decisions? Will this year’s NephMadness finally put an end to this debate?
One of the most challenging aspects of managing patients with ESKD is optimizing their volume status. Currently, no universally-accepted standards exist with which to assess volume status in ESKD. In order to better understand and individualize fluid changes with hemodialysis sessions, a clear understanding of body fluid compartments is needed along with reliable tools for a dynamic assessment of changes in these compartments. The figure below demonstrates the average body fluid compartments in an individual patient:

Schematic of body fluid compartments, prepared by @Stones__ based on figure by @DrTariqShafi
As you think about body fluid compartments, consider these questions: Do you use older or newer methods of volume assessment in ESKD patients? Can you reliably assess body fluid compartments and monitor change during dialysis? Do you think ESKD patients should be kept wetter or drier? Read our scouting reports to help make up your mind.
Old School

Copyright: sorayut / Shutterstock
Old is Gold? Conventional Methods of Volume Assessment in ESKD
Targeting “dry weight,” or the body weight at which a patient has adequate blood pressure control and little to no cramping, edema, or dyspnea, has been a traditional method of assessing a dialysis patient’s volume status. Limitations of relying on this method include dialysis patients’ changes in cell volume driven by age and muscle cell mass, interindividual variability of the fluid content of muscle and fat, and patients’ excess extracellular water content that follows sodium retention.
The physical examination techniques such as jugular venous pressure (JVP) and dependent edema are critical for assessing volume status. A JVP of > 3 cm can reliably measure volume excess post-dialysis. Unfortunately, JVP interpretation may not be reliable in patients with internal jugular vein catheters or other causes such as central venous occlusion. Pedal edema has been shown to correlate more with obesity than excess volume in ESKD. In addition, in the Dry Weight Reduction In Hypertensive Hemodialysis Patients (DRIP) trial, edema was not predictive of a greater decline in blood pressure in response to ultrafiltration.

Visual Abstract by @divyaa24 on Agarwal et al
Blood pressure is also used as a global metric of volume status in dialysis patients. Studies have shown that hypertension in hemodialysis correlates with volume status measured by bioimpedance, particularly when blood pressure measurements are timed appropriately. In an analysis of 30 prevalent hemodialysis patients, ambulatory and post-dialysis blood pressures were more accurate representations of total body volume (measured by bioimpedance) than pre-dialysis blood pressures. However, discrepancies between dialysis unit and standardized blood pressure measurements, alterations according to measurement technique, and changes in measured values as a result of atherosclerosis and vascular calcification may make solely relying on blood pressure for volume status assessment difficult. Despite these limitations, it is difficult to argue against the practical aspects and utility of measuring vital signs when assessing the volume status of an ESKD patient.
Laboratory markers may add additional useful data in the evaluation of a dialysis patient’s volume status. Atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP) are released from cardiac myocytes in response to changes in atrial transmural pressure and increases in ventricular blood volume, respectively. ANP levels have been shown to decrease after hemodialysis and hemofiltration and to remain high in patients with “dialysis-resistant” hypertension, pointing to a potential role for ANP in measuring volume status. However, studies have also shown that ANP levels can remain high in ESKD patients with mitral valve insufficiency or other altered left atrial hemodynamics, making the interpretation of an elevated level challenging. BNP may be a better alternative, as strong relationships have been demonstrated between BNP levels, stroke, myocardial infarction, and mortality in hemodialysis patients. Cyclic guanidine monophosphate (cGMP), produced when ANP activates guanylate cyclase, is more stable at room temperature than ANP and may be another laboratory marker useful in ESKD volume assessment. Though levels are difficult to interpret in the setting of cardiac and valvular dysfunction, cGMP has been shown to correlate well with changes in body weight pre- and post-dialysis.
Central venous pressure (CVP), is considered a good approximation of right atrial pressure, and CVP measurements have long been used to guide volume management in critical care settings. Despite the fact that CVP measurements are invasive and correlate poorly with total blood volume or detect hemodynamic response to a fluid challenge, they may still provide a more accurate assessment of volume status in a dialysis patient than vital signs or laboratory markers alone. Studies have shown that CVP reductions are apparent during the first hour of hemodialysis, pointing to their ability to detect dynamic changes in volume status during dialysis. A non-invasive, yet dynamic method to assess central venous pressure is the use of inferior vena cava (IVC) measurements by ultrasound. Post-dialysis, subdiaphragmatic IVC measurement has been shown to correlate with mean arterial pressure, stroke volume, and heart rate. Additionally, a recent study showed that nurses in dialysis units can reliably perform ultrasound-guided IVC assessments. However, other studies reported a wide range of IVC diameters in the setting of ESKD and cautioned that the presence of tricuspid insufficiency can lead to unreliable results.
Relative blood volume monitoring (RBV), a measurement of changes in hematocrit as fluid is removed from a hemodialysis patient’s vascular space, has also been used to help guide fluid management. During ultrafiltration, there is shift of water from the interstitial fluid compartment to the intravascular compartment (venous and then arterial circuits). Increasing hematocrit implies that the interstitial to intravascular compartment shift is tapering off and that further ultrafiltration could result in decrease in effective circulating volume and intradialytic hypotension. Although initial studies showed good correlation between RBV and extracellular fluid volume, in a subsequent randomized trial of RBV-guided care versus usual clinical care, RBV-guided care was associated with more frequent access-related hospitalizations and higher mortality at six months, and a 22-week randomized crossover trial of RBV-guided ultrafiltration versus usual care showed no differences in intradialytic hypotension, brain natriuretic peptide levels, troponin levels, ultrafiltration rate, or dialysis recovery time during the last week of the study.
When it comes to assessing volume in hemodialysis patients, perhaps old is gold and we should focus on more rigorously evaluating and improving upon our existing measurement techniques as we explore new methods.
New School
Newer is Better: Contemporary Ways to Assess Volume in Dialysis Patients

Copyright: SergeyBitos / Shutterstock
While the physical exam should be part of every patient assessment, its utility may be limited in discerning relatively milder states of volume overload. Dialysis patients may experience intradialytic hypotension for issues unrelated to volume status. Hypotensive episodes in dialysis patients with autonomic dysfunction are caused by a paradoxical fall in sympathetic activity, a reduction in total peripheral resistance, splanchnic venodilation, and reduction in heart rate and cardiac output. Edema may also not be helpful to guide dry weight as edema did not predict a greater antihypertensive response in the aforementioned DRIP trial.
The relative distribution and changes in water content of different body fluid compartments may provide objective data to guide volume management. However, measurement of water in individual body compartments is cumbersome. Estimation of total body water by bioelectrical impedance analysis (BIA) is an alternative to direct measurement. BIA uses electrodes on a patient’s skin to determine the opposition to flow of an electric current. Based on the principle that the electrical impedance of an object is directly proportional to its length and inversely proportional to the product of its cross-sectional area and resistivity, BIA parameters can be used to estimate total body water, intracellular water, and extracellular water. However, BIA cannot distinguish between interstitial and intravascular compartments. Similar to oscillometric blood pressure devices, BIA devices use estimation equations that are often proprietary, limiting direct comparisons between devices.
BIA-guided estimation of fluid compartments has begun to be used in dialysis patients around the world. One study revealed that reductions in dry weight were followed by concordant changes in volume measured by BIA as well as changes in blood pressure. A randomized-controlled trial of 156 dialysis patients showed that BIA-based adjustments in ultrafiltration resulted in regression of left ventricular mass index, decreased blood pressure, and decreased arterial stiffness at one-year follow-up. Currently, the FMC’s Body Composition Monitor is being used in dialysis patients internationally, though it remains unavailable in the US at the time of this writing.
Despite these promising results, challenges to routinely incorporating BIA into clinical practice remain. It is important to note that fluid is distributed unevenly in the body, and whole body BIA is more sensitive to fluid changes in the limbs than in the trunk. Additionally, a qualitative analysis of 24 nephrology healthcare professionals revealed barriers to utilizing BIA in hemodialysis: provider lack of knowledge, awareness, and comfort, as well as concerns regarding workflow, cost, and processes of care.
Still, BIA continues to be used and has been incorporated into 67 randomized controlled trials (6 ongoing) to guide fluid management in hemodialysis. While some studies have shown that BIA-guided dry weight prescriptions resulted in a 90% risk reduction in all-cause mortality over two-and-a-half year of follow-up as well as a lower odds of post-dialysis hypotension, other analyses have highlighted limitations, including a lack of an improvement in preservation of residual kidney function or echocardiographic parameters over one-year follow-up using BIA-guided volume management in peritoneal dialysis.
Lung ultrasound can also objectively quantify pulmonary vascular congestion. B-lines on lung ultrasound are vertical, hyperechoic, dynamic lines that originate from the pleura and can be indicative of alveolar edema. Serial lung ultrasound measurement of B-lines can provide a dynamic assessment of volume shifts during dialysis. Intradialytic changes in B-lines correlate with the percent change in a patient’s total body weight and ultrafiltration rate. Lung ultrasound may also be more sensitive than chest x-ray, as seven out of ten patients with clear pre-dialysis chest x-rays exhibited B-lines on lung ultrasound. Very severe pulmonary congestion seen on B-line guided lung water assessment predicted an increased risk of death and adverse cardiovascular events at two-year follow-up in a multi-center study of 392 patients with ESKD.
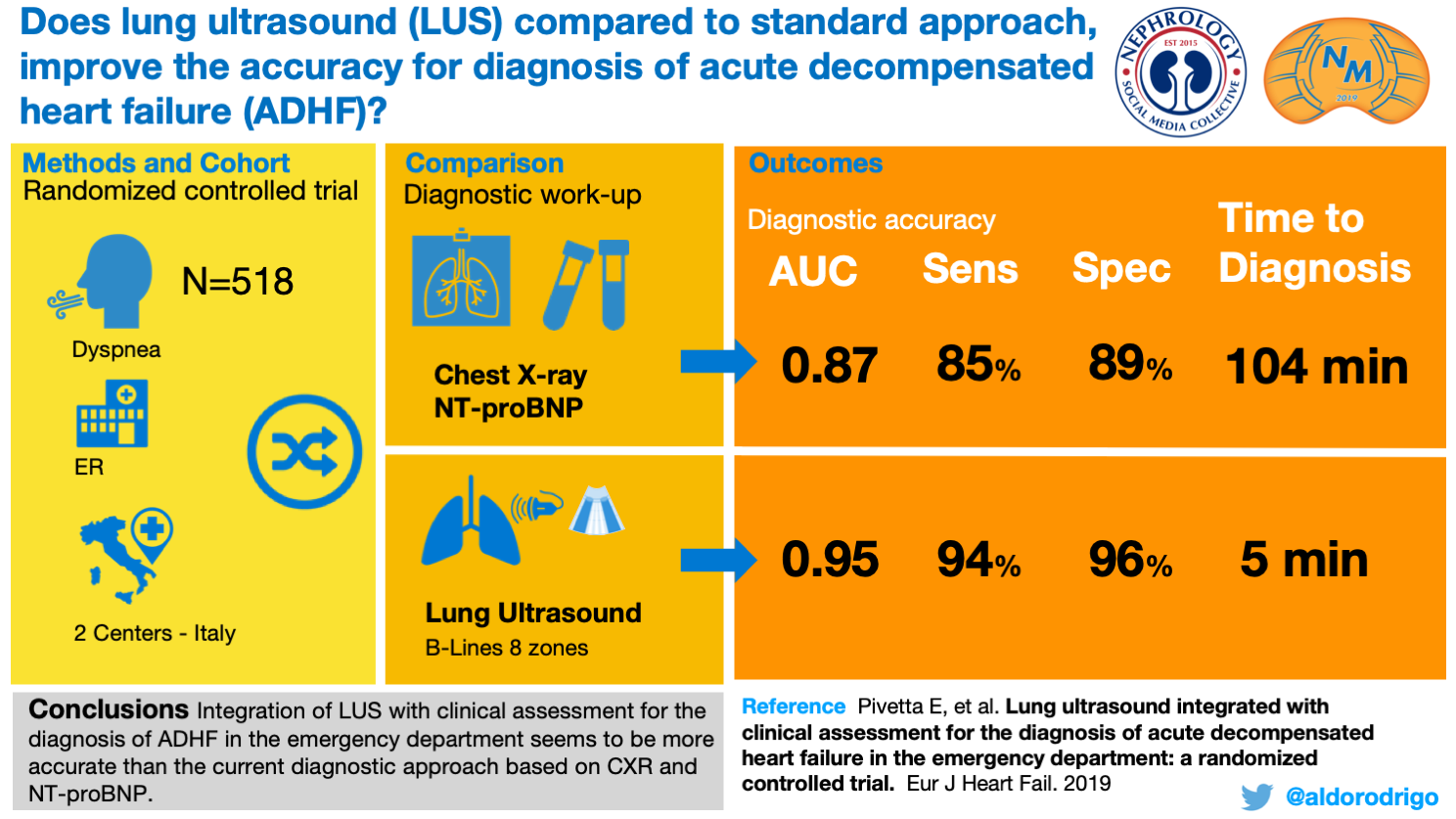
Visual Abstract by @aldorodrigo on Pivetta et al
So, how do these methods compare? A sub-study of the ongoing Lung Water by Ultrasound Guided Treatment to Prevent Death and Cardiovascular Complications in High Risk ESRD Patients with Cardiomyopathy (LUST) Trial demonstrated that lung congestion by crackles or edema poorly reflected the severity of congestion reflected by B-line scores.

Visual Abstract by @vandyniyyar on Torino et al
In another study that compared 53 ESKD patients’ B-line scores, BIA measurements, and blood volume monitoring to assess volume, B-line scores showed the greatest sensitivity and specificity.

Visual Abstract by @Buck1486 on Alexiadis et al
While lung ultrasound seems to be superior, a randomized controlled trial of 250 hemodialysis patients compared LUS and BIA measurement-guided dry weight adjustments with usual care and found no changes in all-cause or cardiovascular mortality at 21 months. However, as previous myocardial infarction, heart failure, active infection, or malignancy were excluded, patients were considered lower-risk at baseline and may not have needed protocolized dry weight adjustments.
BIA and LUS have the most research to date but newer, more sophisticated techniques are becoming available. There is an ongoing, prospective study of ESKD patients using non-invasive measurements of left-ventricular end-diastolic pressure (LVEDP) to guide volume management. Alterations in LVEDP are recorded by Valsalva-induced changes in the pulse amplitude of finger photoplethysmography (PPG) probes. Preliminary results have shown that LVEDP is lower in patients with symptomatic intradialytic hypotension, suggesting that non-invasive LVEDP measurement may be an additional tool to measure volume status in ESKD. Cheetah sensors use alternating current to detect changes in stroke volume using sensor pads applied to a patient’s chest and could theoretically be used to provide dynamic non-invasive hemodynamic monitoring during dialysis. Devices such as wearable ultrasound patch and oral sodium sensors are in early stage of development. The wearable ultrasound patch is a tiny, flexible skin patch that uses transducers to detect volume-related changes in blood vessel diameter. Oral sodium sensors use Bluetooth technology to transmit data regarding sodium ion content in food to a tablet or smartphone app.
Are these the newer, better methods of volume assessment that we should be turning our attention to?
Dry on Dialysis vs Wet on Dialysis

Wet on Dialysis vs Dry on Dialysis. A conceptual Model of Outcomes Associated with Volume Status Changes in Hemodialysis, prepared by @Stones__ based on figure by @DrTariqShafi
Dry on Dialysis

Copyright: Paul Vinten / Shutterstock
Less Wet is More: Achieving a Target Weight and Limiting Interdialytic Weight Gain
Studies show that volume overload is harmful. Volume overload can lead to arterial stiffness, hypertension, and left ventricular hypertrophy from neurohumoral alterations such as higher levels of circulating catecholamines and activation of the renin-angiotensin system.
Volume overload increases mortality and cardiovascular events. A retrospective analysis of 34,107 dialysis patients found that patients with an interdialytic weight gain of over 4 kg above their dry weight had a 28% and 25% increased risk of all-cause and cardiovascular mortality, respectively, even after adjusting for demographics and surrogate markers of malnutrition and inflammation. Numerous other observational studies have demonstrated the adverse cardiac and cerebrovascular events associated with excess interdialytic weight gain. The Prevalence of Precapillary Pulmonary Arterial Hypertension in Patients with End-Stage Renal Disease (PEPPER) study revealed that persistent volume overload post dialysis sessions contributed to pulmonary hypertension.

Visual Abstract by @PabloGarciaMD on Kalantar-Zadeh et al
Volume overload also increases hospitalizations. A recent retrospective cohort of 113,561 prevalent ESKD patients showed those with a post-dialysis weight of 1 kg above estimated dry weight had more frequent emergency department visits and cardiovascular-related hospitalizations, in addition to increased all-cause mortality.
Volume overload is clearly associated with worse outcomes in ESKD, but it may also be important to consider patients’ symptoms and priorities before adjusting dialysis prescriptions – read on and hear the patient perspective before you make your choice.
Wet on Dialysis

Copyright: Lorenzooooo / Shutterstock
More Wet is More: Valuing Patient-Reported Outcomes
Few may be able to argue with the importance of aggressively challenging dialysis patients’ dry weights… except perhaps our patients themselves. The Standardized Outcomes in Nephrology – Hemodialysis (SONG-HD) initiative, an international survey project consisting of 1,181 participants from 73 countries, asked patients, caregivers, and health professionals to rank health outcomes according to personal preference and research priority. Results showed significant discordance between provider and patient/caregiver preferences. Providers prioritized mortality, hospitalizations, and blood pressure reductions, whereas patients and caregivers emphasized the importance of treating fatigue, maintaining energy, and promoting healthy coping behaviors. The table below shows the divergence in outcomes of greatest importance from Patients/Caregivers and Health Professionals.

Table 1 from Speyer et al, AJKD, © National Kidney Foundation.
While achieving euvolemia is often considered an important goal of dialysis, excessive volume removal and intradialytic hypotension in the setting of dialysis can cause major adverse objective outcomes such as myocardial stunning, stroke, arteriovenous fistula complications, a steeper decline in residual kidney function, and higher mortality.
Aggressively reducing dry weight also causes increased cramping and fatigue. Patients in the intervention arm of the DRIP trial experienced more frequent intradialytic cramps, lightheadedness, and hypotensive episodes. This leads to decreased patient satisfaction.
So, should improvements in objective markers of volume status be targeted if patients do not experience subjective benefits? Ultrafiltration prescriptions should not be ‘one-size-fits-all.’ Patient comorbidities and disease characteristics dictate the level of vascular filling from the interstitium and what a patient is likely to be able to tolerate. Ultimately, aggressively challenging a patient’s dry weight should not come at the expense of dialysis adherence or patient discomfort.
– Executive Team Member for this region: Anna Burgner, AJKD Social Media Advisory Board member. Follow her @anna_burgner.
How to Claim CME and MOC
US-based physicians can earn 1.0 CME credit and 1.0 MOC point for reading this region.
- Register/log in to the NKF’s Professional Education Resource Center (PERC).
- Review the activity and accreditation information.
- Click “Continue” and review Course Instructions.
- Complete Post-Test. Please note: By selecting “Yes” to the participation questions for each region, the corresponding Post-Test questions will appear. Click “Save Draft” to save your responses and finish later. When you are ready to submit your answers, click “Preview” to review all responses, then click “Submit.”
- Click “Next” to complete the Evaluation form, then click“Submit.”
- Claim 1.0 CME credit and 1.0 MOC point per region (up to 8.0 total for 8 regions of NephMadness).
- Print your certificate.
- Review the Post-Test answers and rationale.
The CME and MOC activity will expire on June 15th, 2019.

Thank you. It is very interesting update