
Contrast-Induced Nephropathy: Does It Really Exist?
Many different definitions of contrast-induced nephropathy (CIN) have appeared in the literature since it was first reported in 1954. It is commonly defined as an acute decline in kidney function following the administration of intravenous iodinated contrast in the absence of other causes. For research purposes, a definition such as a rise in serum creatinine (Scr) ≥ 25 or 50% above the baseline value is often used. Patients often typically present with an acute rise in Scr 24-48 hours post-contrast exposure. Scr generally peaks at 3 to 5 days and then returns to baseline value by 7 to 10 days. The acute kidney injury (AKI) is non-oliguric in most cases with urinalysis often revealing granular casts, tubular epithelial cells, and minimal proteinuria, but in many cases may be entirely bland. Most, but not all, patients exhibit low fractional excretion of sodium due to afferent vasoconstriction. The diagnosis of CIN is frequently obvious if the typical course of events follows the administration of contrast.

Image from Shutterstock / pang_oasis
Known risk factors for CIN can be divided into those that are patient-related (underlying CKD, older age, female gender, diabetes, proteinuria, intravascular volume depletion, decreased cardiac output, and co-administration of nephrotoxic agents), and those that are procedure-related (increased dose of contrast media, multiple procedures within 72 hours, intra-arterial administration, as well as type of contrast media used). From the pathophysiological standpoint, contrast media leads to nephropathy via induction of medullary hypoxia (intrarenal vasoconstriction, altered blood rheology, osmotic load), which leads to generation of reactive oxygen species as well as via direct tubular toxicity.
Preventive strategies described in literature include: selection of contrast agent (non-iodinated, iso-osmolar), volume administration, pharmacologic therapy, hemodialysis and hemodialfiltration, as well as avoidance of co-administration with other potentially nephrotoxic agents.
Despite the above, in 2017, the AMACING trial concluded “no prophylaxis to be non-inferior and cost-saving in preventing contrast-induced nephropathy compared with intravenous hydration according to current clinical practice guidelines.” There are admittedly several issues with this study. Since then, there have been countless meta-analyses of the data over the years that have also reached the opposite conclusion. There have also been several publications that question the true existence of CIN.
A recent AJKD In Practice by Rudnick et al (freely available until Feb 29, 2020) was commissioned to celebrate the selection of Iodinated Contrast as a finalist in NephMadness 2018.

Visual Abstract by @JamesNovakNeph
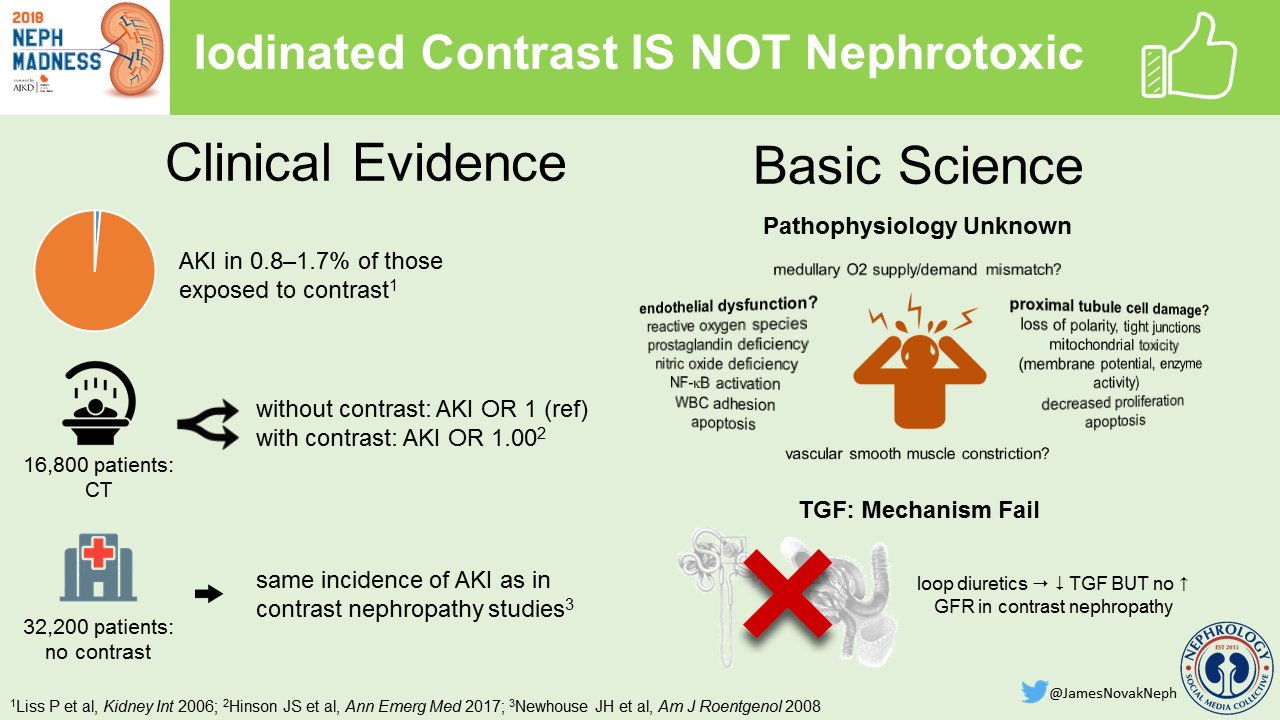
Visual Abstract by @JamesNovakNeph
Rudnick et al provide a comprehensive review of the literature highlights the significant heterogeneity of the different studies, and also their strengths and limitations. Considering the imbalance in confounding covariates and selection bias between studied populations, the authors point out that “the ideal approach to determine CIN following intravenous contrast would be a randomized controlled trial (RCT) in patients undergoing computed tomography (CT) with or without contrast media enhancement,” thereby ensuring balanced comorbid conditions between groups and non-biased randomization. For ethical and logistical reasons, it is unlikely that such RCTs will be performed. Recognizing these limitations, several studies using propensity score matching methods are presented in Table 1 below.

Table 1 from Rudnick et al AJKD © National Kidney Foundation.
Existing evidence points to a negligible risk for CIN following intravenous contrast exposure in patients with eGFRs ≥ 60 mL/min/1.73 m2 or mildly decreased kidney function (eGFRs of 45-59 mL/min/1.73 m2). It also seems clear that patients with eGFRs < 30 mL/min/1.73 m2 are at greatest risk for CIN following intravenous CM exposure, despite mixed findings of the propensity score studies.
In conclusion, Rudnick et al make several recommendations:
- A single eGFR determination should not be the sole basis for risk classification for AKI following exposure to contrast media. This is particularly true for those with eGFRs of 30 to 45 mL/min/1.73 m2 and in some with eGFRs < 30 mL/min/1.73 m2. It is also important that the patient has a stable Scr level prior to exposure to contrast media. Physicians need to consider patients’ individual unique risk factors for CIN and balance the risks and benefits following exposure to contrast.
- A team-approach is of utmost importance. Discussions between radiologists and physicians ordering CT on the added clinical value of contrast requiring procedure.
- In patients deemed at high risk for CIN, alternative non-iodinated contrast studies (contrast-enhanced ultrasound or MRI with newer gadolinium-based contrast agents) should be considered as they may provide adequate diagnostic information while negating the risk for nephrotoxicity.
- In patients deemed at high risk for CIN, whereby contrast enhanced imaging study is deemed absolutely necessary, it is important to render renal prophylaxis measures with saline solution hydration and techniques to minimize contrast volume.
- More adequately powered propensity score studies need to be conducted in those with eGFRs < 45 mL/min/1.73 m2 with and without DM to further clarify the true risk for CIN in these presumed at-risk patients.
So, does CIN exist? The word “renalism” was coined by Dr Glenn Chertow @gchertow to refer to the failure to perform appropriate diagnostic/therapeutic interventions in patients with CKD due to concern about risk of AKI. Aversion to the risk of contrast nephrotoxicity is inappropriate if the benefit of the exposure far outweighs the minimal risk.
Rather than rehash the conclusions, Dr Steven Weisbord @stevenweisbord presented this nice summary during ASN Kidney Week 2017:

Reproduced with permission from @stevenweisbord
– Post prepared by Trisha Patel (PGY-2, Internal Medicine, UIC/Advocate Christ Medical Center), AJKDBlog Guest Contributor, and Edgar Lerma @edgarvlermamd, AJKD Social Media Advisory Board member.
To view Rudnick et al (FREE until Feb 29, 2020), please visit AJKD.org.
Title: The Controversy of Contrast-Induced Nephropathy With Intravenous Contrast: What Is the Risk?
Authors: Michael R. Rudnick, Amanda K. Leonberg-Yoo, Harold I. Litt, Raphael M. Cohen, Susan Hilton, and Peter P. Reese
DOI: 10.1053/j.ajkd.2019.05.022
Leave a Reply