
Hemodialysis Access Shared Decision Making
Melandrea Worsley @MWorsleyMD
Dr. Melandrea Worsley is a current nephrology fellow at Baylor College of Medicine in Houston, Texas. She is passionate about addressing disparities in hemodialysis vascular access.
L. Parker Gregg @LParkerGregg1
Dr. L. Parker Gregg is an Assistant Professor at Baylor College of Medicine, the Michael E. DeBakey VA Medical Center, and the Center for Innovations in Quality, Effectiveness and Safety. Her primary interests are in non-traditional risk factors in CKD.

For patients with kidney failure who require hemodialysis (HD), vascular access becomes their lifeline. Obtaining and maintaining vascular access with an arteriovenous fistula (AVF), arteriovenous graft (AVG), or a central venous catheter have unique risks and benefits. The risks associated with the creation and maintenance of an AVF or AVG include bleeding, nerve damage, maturation failure, infection, steal syndrome, and high-output heart failure.[1] These vascular accesses can be complicated by clotting, stenosis, aneurysms, or pseudoaneurysms, which can require additional procedures to maintain access patency and function.[2] Dialysis catheters, on the other hand, are considered to have a higher risk of bloodstream infections, may achieve slower blood flow rates with effects on clearance, and can have problems of patency that require placement of a new catheter.[3]
Prior clinician-driven policies focused on a fistula-first approach to creating HD vascular access, with the rationale that AVFs were thought to have fewer complications than other vascular access types. In 2003, the Centers for Medicare and Medicaid Services (CMS) assembled a task force of vascular access experts, nephrologists, and nurses for the Fistula First National Vascular Access Improvement Initiative. This group was formed to develop and implement systemic changes to support the creation of AVFs for HD. This practice pattern revealed high rates of AVF maturation failure. To address this, in 2015 the Fistula First Catheter Last Workgroup Coalition was formed to reduce the number of catheters that were being used for HD access, as well as to implement further systemic changes needed to increase the rate of successful AVF creation. Despite initiatives and incentives put into place to decrease catheter use, between 2009 and 2018 the rate of HD initiation with a catheter only decreased from 82.4% to 80.8%. Among patients who initiated HD in 2017, 68% of patients were still dialyzing via a catheter 3 months after initiation.[4] More recently it has been recognized that many patient-level factors also affect HD vascular access decision-making. Consequently, a more patient-centered approach of individualized decisions about vascular access in the context of strategizing for living with kidney failure is now recommended.[5]
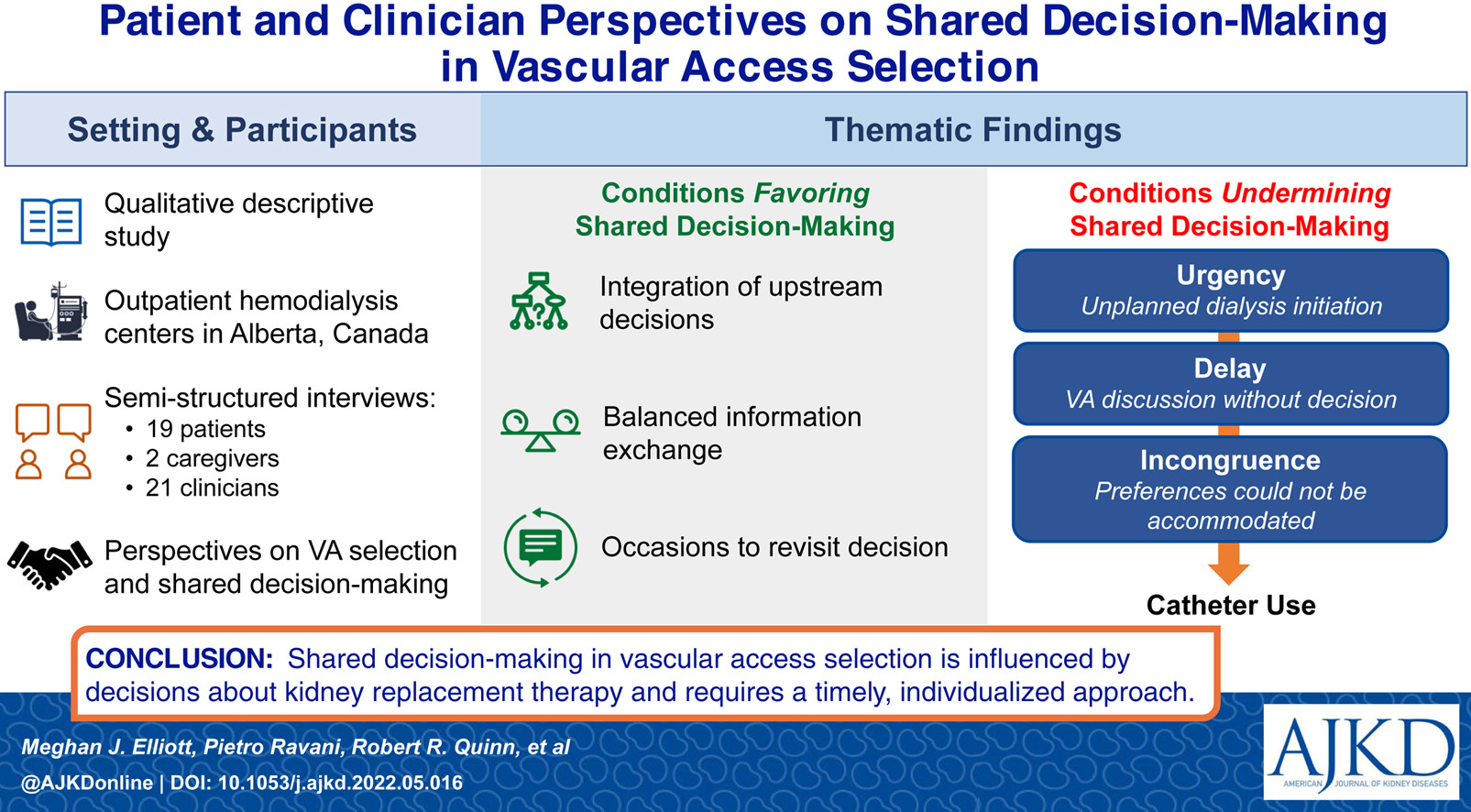
In a recent qualitative study, Elliott et al interviewed 19 patients on chronic HD, two caregivers, eight nephrologists, and 13 HD or vascular access nurses at five adult in-center HD units in Alberta, Canada to better understand how these groups perceive the process of shared decision making about vascular access. They identified that shared decision-making about vascular access begins with foundational conversations about prognosis and dialysis modality, which should incorporate the patient’s values, abilities, and priorities. This puts future conversations about vascular access into a meaningful context. The authors note that the process of shared decision-making was undermined in cases of unplanned dialysis initiation, lack of a decision about vascular access prior to the need to start dialysis, or an inability to achieve the patient’s desired vascular access type. This analysis demonstrates that multiple important decisions, beginning with goals of care and prognosis, set the stage for effective shared decision-making about vascular access. Repeated discussions are often necessary, and a patient’s decision about vascular access can be readdressed even after HD initiation.[6]

Figure 1. Factors impacting HD vascular access shared decision making.
Discussions concerning vascular access placement should incorporate patient education about factors that may influence this decision, while also encouraging patients to educate clinicians on their personal healthcare priorities. Several crucial factors impact the decision-making process, including the timing and context of discussions of prognosis and vascular access, patient priorities, biological and surgical factors, and sociocultural considerations.
As for the timing of these discussions, it may be difficult for clinicians to anticipate the amount of time a patient has prior to initiating dialysis, which can complicate pre-dialysis planning. In some cases, depending on the patient’s rate of decline in kidney function, a late referral to nephrology when estimated glomerular filtration rate (eGFR) is already low may not provide adequate time for a patient to accept that they may ultimately need dialysis, determine their desired dialysis modality, and have a vascular access placed and ready to use in time. Acute kidney injury may necessitate dialysis initiation sooner than anticipated. In such cases, patients may pursue urgent HD with a catheter as their only available option at the time of initiation.
Patients’ personal healthcare priorities must also be considered when vascular access is selected. A trusting clinician-patient relationship that enables the patient to safely express their priorities is key. Patients’ individual goals should be considered; for example, those who anticipate forthcoming kidney transplantation may elect to defer AVF placement given the brief expected time on HD. Patients’ concerns, such as fear of needles or cosmesis, must be considered as well. Surgical placement of a vascular access results in scarring, and over time AVFs may enlarge having an undesirable cosmetic effect. Priorities such as these may have striking impact on a patient’s decision-making process and should be acknowledged by clinicians and incorporated into patient-centered discussions.
Biological and surgical factors also contribute to the patient’s eligibility for vascular access creation and can undermine shared decision-making when a patient is not able to receive their preferred access type. In order for an AVF to be placed, a patient must have adequate vasculature to allow for access placement and maturation. Many patients have insufficient vasculature due to comorbidities, such as diabetes mellitus and hypertension.[7] Access to experienced surgeons may also impact decision-making about access eligibility. In one study, surgeons with more than 30 years of clinical experience and vascular surgeons (vs. general or cardiothoracic surgeons) were more likely to place an AVG as a patient’s initial HD access, independent of patient-level factors.[8]
Sociocultural factors may also influence the type of HD access a patient receives. For example, racial and ethnic healthcare disparities have been identified regarding HD vascular access. Black patients are less likely to receive an AVF and more likely to require a second access when compared to White patients.[9] Black patients are also less likely to initiate HD with an AVF, despite being younger and having less coronary artery disease, when compared to White patients.[10] Black patients are less likely to receive nephrology care prior to kidney failure when compared to their White counterparts, which likely contributes to these disparities. Education level, employment status, and the availability of caregiver support may also impact vascular access decision-making. Further qualitative research will be important to understand the extent to which such sociocultural factors influence HD vascular access decision-making.
The nature of vascular access decision-making is complex and requires integration of that decision into repeated conversations starting from the foundational discussions about prognosis to help patients understand and accept the need to plan for dialysis. Prior policies prioritizing one access type over another did not account for this complexity, which may have contributed to the less-than-anticipated success in reducing the use of dialysis catheters. The analysis by Elliot, et al. suggests we should integrate the vascular access decision process into earlier discussions and consider the upstream clinician-patient relationships and conversations that lay the critical foundation for vascular access shared decision-making. Thoughtful communication between clinicians and patients is important to individualize vascular access decision-making and ensure that patients’ priorities and goals are considered in their care plan. The shift toward individualized vascular access decisions represents a patient-centered transition in thinking that will ultimately improve the quality of care that is provided to patients with kidney failure.
–Post prepared by Dr. Melandrea Worsley @MWorsleyMD and Dr. L. Parker Gregg @LParkerGregg1
To view Elliott et al (FREE temporarily), please visit AJKD.org.
Title: Patient and Clinician Perspectives on Shared Decision-Making in Vascular Access Selection: A Qualitative Study
Authors: Meghan Elliott, Pietro Ravani, Robert Quinn, Matthew Oliver, Shannan Love, Jennifer MacRae, Swapnil Hiremath, Sarah Friesen, Matthew James, and Kathryn King-Shier.
DOI: 10.1053/j.ajkd.2022.05.016
Leave a Reply