
Towards Sex and Gender Equity in Kidney Care and Research
Jeffrey Ha @_jeffreyha
Dr. Jeffrey Ha is a nephrologist in the Sydney Local Health District. He attended medical school at University of Sydney and completed his nephrology training in the East Coast Renal Network in Sydney. He is currently undertaking a PhD through The George Institute for Global Health, to better understand and manage the high burden of cardiovascular disease in patients with chronic kidney disease (CKD). His research interests are in epidemiology, clinical trials, and expertise in anticoagulation and the treatment of cardiovascular disease in CKD.
Carinna Hockham @carinnahockham
Dr. Carinna Hockham is a kidney disease epidemiologist at The George Institute for Global Health, Imperial College London. Her research interests lie in the sex and gender differences (and similarities) in chronic kidney disease and, more recently, multimorbidity.

Sex is a biological construct, defined by our complement of chromosomes at birth, with the physiological influences of our gonads and sex hormones throughout life. Gender, by contrast, is attributed to the social, environmental, cultural, and behavioral factors that influence our identity. Although often used interchangeably due to their high degree of congruence in the population, sex and gender are distinct concepts and should be considered accordingly.
Differences in the burden, progression, and outcomes of kidney disease between females and males and women and men are known to exist. A Special Issue in Seminars in Nephrology states that it is time for a paradigm shift in kidney care and research, which fundamentally “[addresses] the specific sex- and gender-based differences in the physiology, pathophysiology, presentation, choice of therapies, and response to treatments”.
There is a growing body of literature detailing the sex- and gender-based differences and disparities in kidney care and research. Figures 1 and 2—whilst not exhaustive—highlight important differences and disparities between males/females and men/women across the spectrum of kidney disease.
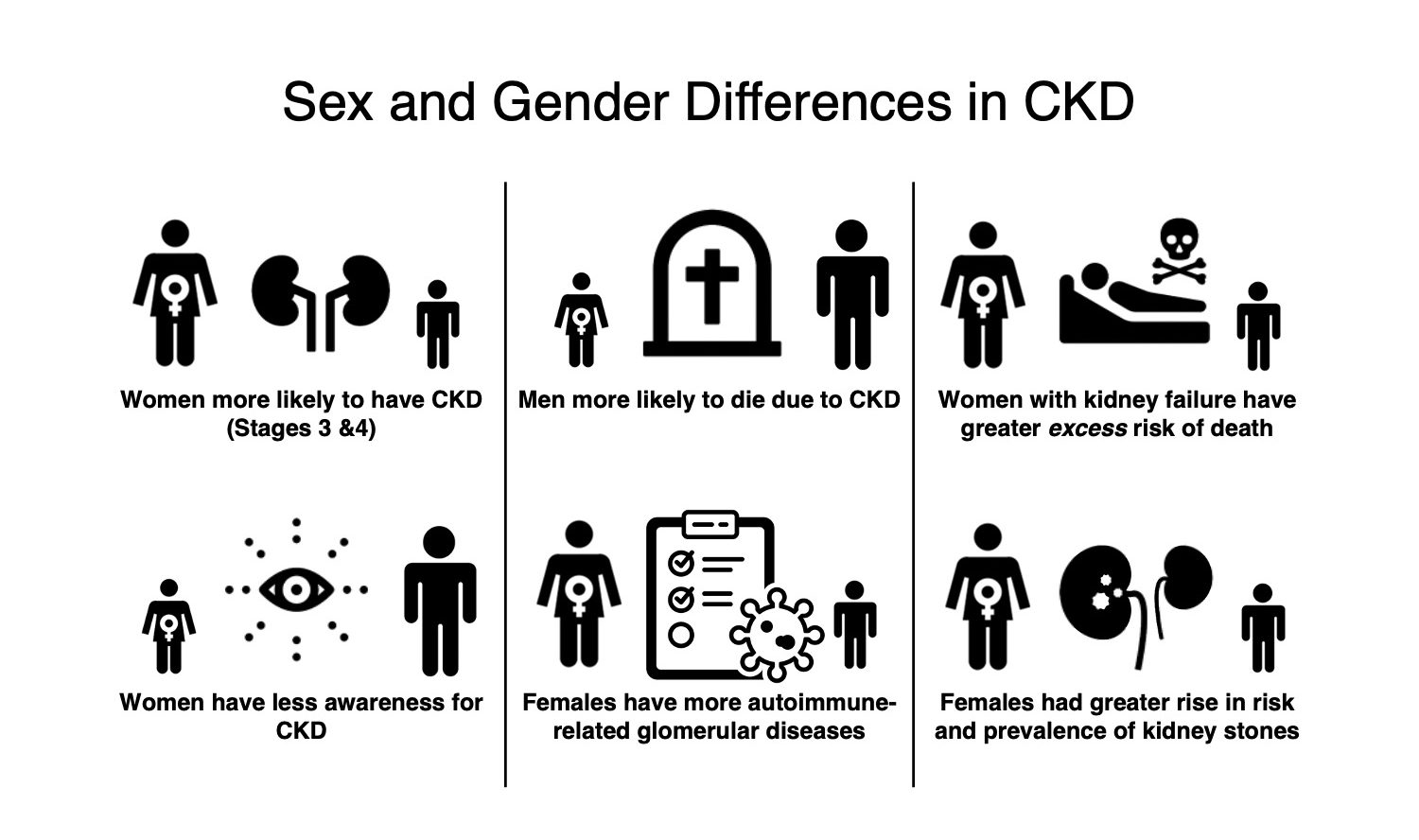
Figure 1 © Jeffrey Ha and Carinna Hockham

Figure 2 © Jeffrey Ha and Carinna Hockham
Notably, these do not highlight the barriers to healthcare and adverse outcomes that transgender, nonbinary, or gender-diverse people face, which are instead nicely summarized in this review. The visual abstract in a review from Drs. Katz-Greenberg and Shah also beautifully illustrates some of the sex and gender differences that are present in kidney transplantation (Figure 3).

Sex and gender differences in kidney transplantation. Figure 1 from Katz-Greenberg et al, Seminars in Nephrology This is an open-access article distributed under the terms of the Creative Commons CC-BY license.
The meta-epidemiologic study from Dr. Collister et al. on sex and gender in randomized controlled trials (RCTs) involving adults receiving maintenance dialysis is therefore timely. 561 RCTs published in high-impact journals over the last two decades were included.
Key findings
- The RCTs were representative of the general dialysis population with regards to the percentage of females/women in trials (nearly 40% which is consistent with observational data from DOPPS and USRDS). This is in contrast to a previous meta-analysis which suggests that men are more likely than women to be represented in dialysis trials relative to their distribution in the US dialysis population.
- The study did not identify a trial characteristic associated with a greater percentage of female/women participants, apart from the percentage of female/women participants being marginally higher in studies conducted in Asia.
- Sex and gender were reported inconsistently in dialysis trials. Around a third (31%) did not explicitly report the sex or gender of their participants (i.e., did not specifically use the term sex and/or gender but used the descriptors “male/female” or “man/woman” without referring to sex or gender specifically).
- Where the terms “sex” or “gender” were used, authors in the included studies tended to prefer the term sex over gender in recent years.
- The RCTs often did not consider sex or gender in their study design, possibly to the detriment of women. Sex- and/or gender-biased exclusion criteria were commonly used (in 27% of RCTs; usually to exclude female participants based on child-bearing potential, or with stringent contraception requirements) and rarely used as inclusion criteria (3%).
- Sex- and gender-specific outcomes in dialysis RCTs were infrequently reported, and only 16% of studies performed subgroup analyses adjusting for treatment effects according to sex or gender.
What does this study NOT address?
- The study could explore further whether the proportion of females/women in dialysis trials was related to the type of interventions studied (i.e., pharmacological interventions versus non-pharmacological, behavioral interventions, of which the latter may be more likely to attract women).
- Given that sex and gender are often used interchangeably, the correct use of sex and/or gender relative to the descriptors “female/male” and “women/men” was not assessed. Given the different implications that sex- versus gender-based differences might have on our understanding of kidney disease and intervention design, this distinction is important and their interchangeable use highlights a knowledge gap.
- The study also did not include trials with kidney transplant recipients, nor the wider CKD population (which would be an ambitious study!). As a point of reference, a scoping review by Laprise et al. of transplant studies showed that sex or gender was usually applied erroneously or used interchangeably, and only 15% of studies considered sex or gender in the study’s primary question. Most of these studies considered sex and gender variables as confounders, with few studies considering them as modifiers of treatment effects.
What are the implications for clinical practice and future research? How do we remove barriers towards participation of more females/women in kidney research?
Although not directly related to the study’s findings, the paper gives several useful recommendations and future directions for incorporating sex and gender in research involving patients with kidney disease (which are also listed in the accompanying Visual Abstract).
Specific targets to recruit more females/women into nephrology trials may need to be adopted, especially if sex/gender is likely to modify the effect of the intervention. At the very least, the study population should be proportional to and reflect the gender distribution of the target population with the condition, to maintain the generalizability of the study’s results. Inclusivity with regards to transgender, non-binary and gender diverse individuals will also be important. A risk-based approach to eligibility criteria based on sex or gender should also be implemented (so females of child-bearing age for example, should not be excluded by default).
Sex and gender differences should not pose barriers to accessing nephrology care. A better understanding of sex- and gender-specific differences and disparities warrants further research. This enables us to improve outcomes and move towards equity for patients across the spectrum of kidney disease.

– Post prepared by Jeffrey Ha and Carinna Hockham
To view Collister et al, please visit AJKD.org.
Title: Sex and Gender in Randomized Controlled Trials of Adults Receiving Maintenance Dialysis: A Meta-epidemiologic Study
Authors: David Collister, Lonnie Pyne, Arrti A. Bhasin, Sofia B. Ahmed, Brendan Smyth, William Herrington, Meg Jardine, and Michael Walsh
DOI: 10.1053/j.ajkd.2022.10.015
Leave a Reply