
C4 Glomerulopathy: Should We Accept it As a New Disease?
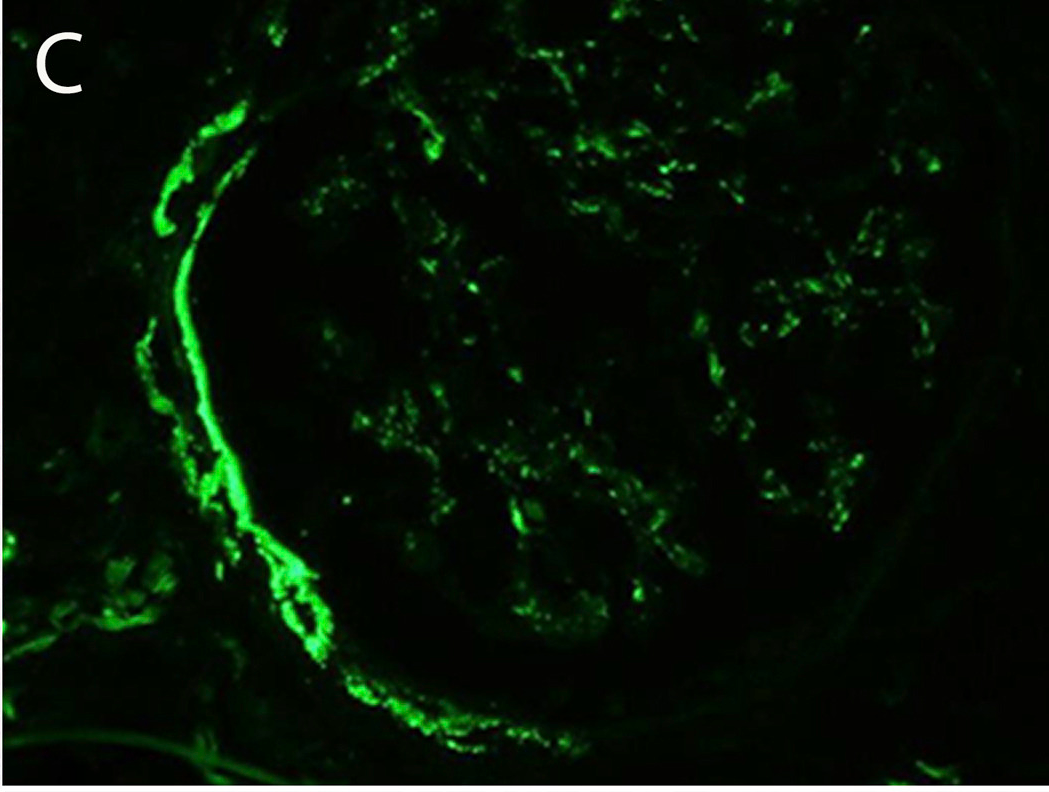
Immunofluorescence microscopy shows trace C3 staining in the mesangium and few capillary walls. Fig 1C from Sethi et al AJKD, © National Kidney Foundation.
A recent article published by AJKD reports 3 patients with nephrotic syndrome, two of whom also had hematuria. Kidney biopsy revealed mesangioproliferative glomerulonephritis in one case, membranoproliferative glomerulonephritis in the second case, and dense deposit disease in the third. In all cases, predominant C4d staining was observed in the glomeruli under immunofluorescence. The term C4 glomerulopathy has been coined for these cases.
C4 deposition often reflects activation of the classical complement pathway. If this were so, we would also expect to find deposition of C3. However, that was not the case, and raises the question whether the lack of detection of C3 or immunoglobulins is due to technical factors. One possibility is the presence of cryptic epitopes not unmasked by pronase digestion. Another potential variable is that C4d is an inherently more stable molecule than C3, and better survives suboptimal fixation.
While evaluating the proposed term C4 glomerulopathy, it should be kept in mind that ‘trace’ mesangial staining for C3 was in fact recorded in two cases. A C3 spectral count of 9 for patient 1 is of the same order of magnitude as the spectral count of 12 for C4b in that biopsy. The presence of ‘no or minimal’ immunoglobulin is also acknowledged in all cases, and this means that at least 4 spectral counts were present. Spectral counting is not a very accurate technique for quantification of proteins, and differences of less than 1 log may not be meaningful.
It is worth noting that a broad range of immunofluorescence findings is acceptable in many well described clinical entities in renal pathology. Therefore, a difference in immunofluorescence staining pattern alone should not be accepted as the basis for defining a new glomerular disease. For example, in IgA nephropathy, about 25% of cases show exclusively IgA deposits in the glomeruli, while 75% also show IgG and IgM. Similarly, while 95% of biopsies show only C3 deposition, the remaining 5% also show C4 or C1. To give another example, while most cases of lupus nephritis show prominent C1q deposition, there is a subset of patients that does not. Differences in stages of the same disease can account for some of this variation in pathology findings.
In summary, the reported cases are indeed very interesting and merit more study. However, before accepting these patients as examples of a new clinical entity, it would be desirable to build up a larger experience and show that the etiology, clinical course, and/or outcome differ from existing clinico-pathologic entities. The latter include immune complex mediated membranoproliferative glomerulonephritis with a broader spectrum of immune reactants and dense deposit disease where primarily C3 is detected.
Notwithstanding these considerations, the authors make a very sound recommendation that ordering a C4d stain may help establish the diagnosis of immune complex glomerulonephritis in biopsies where the standard immunofluorescence panel is negative, but ultrastructural examination shows electron dense deposits.
Parmjeet Randhawa, MD
AJKD Blog Contributor
To view the article abstract or full-text (subscription required), please visit AJKD.org.
Leave a Reply