
#KidneyWk 2016: A Focus on Renal Fellow Education
Newer innovative teaching methods have several advantages over traditional lectures and powerpoints. Examples of effective clinical education tools such as team based learning or case-based debates can be used to great effect to enhance medical education at multiple learner levels.
 During the morning of day 2 of #KidneyWk, AJKD Blog contributors, Dr. Kenar Jhaveri and Dr. Hitesh Shah, along with nephropathologist, Dr. James Pullman, moderated the 5th Annual ASN Kidney Week Fellows-In-Training Bowl using case-based debates.
During the morning of day 2 of #KidneyWk, AJKD Blog contributors, Dr. Kenar Jhaveri and Dr. Hitesh Shah, along with nephropathologist, Dr. James Pullman, moderated the 5th Annual ASN Kidney Week Fellows-In-Training Bowl using case-based debates.
THE RULES:
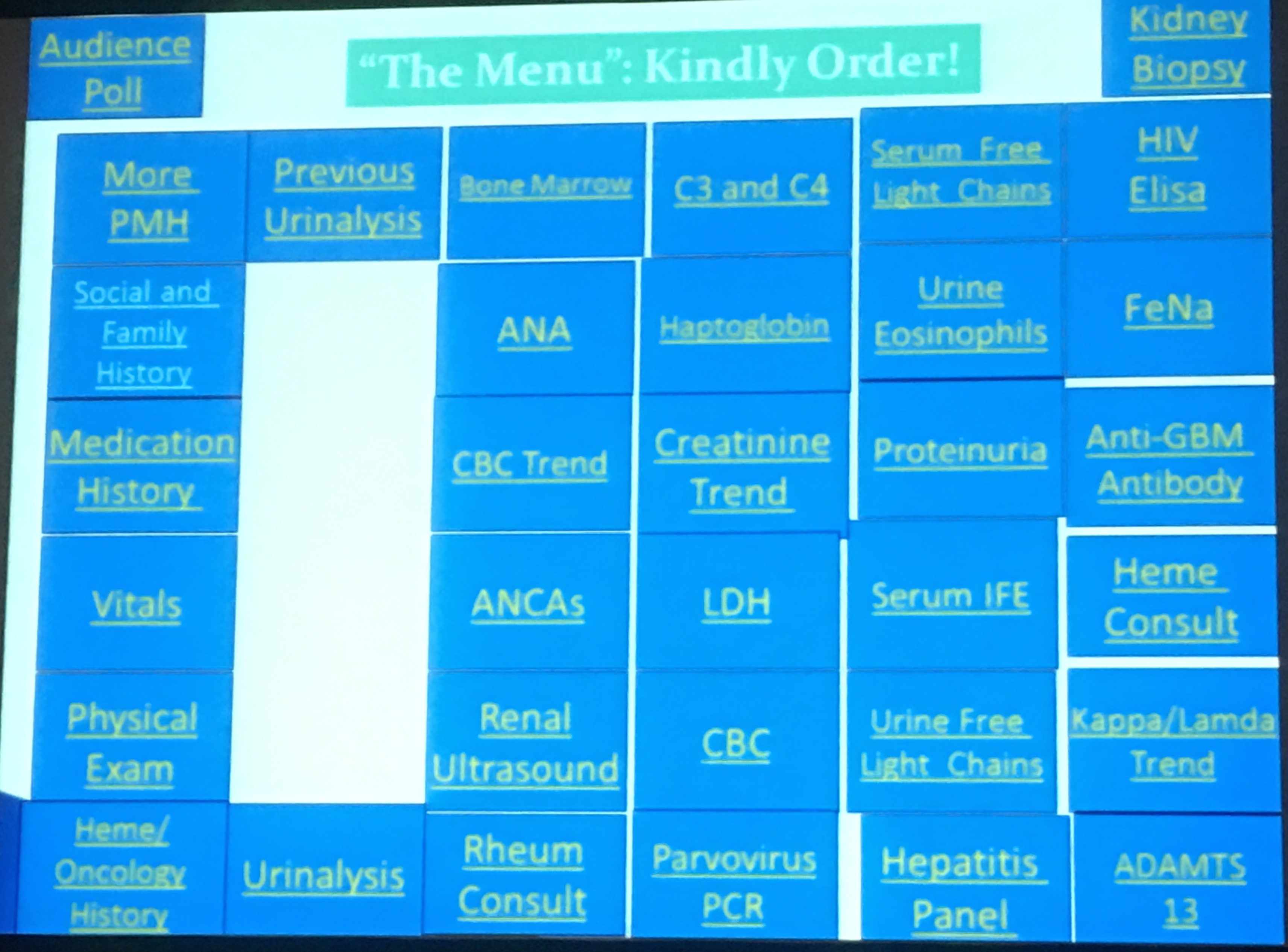
A case would be presented, and teams would go back and forth requesting more information and ordering tests from a menu of options (see image). Every request would require an explanation for why it was being done, and the appropriateness of each test selected would earn the team points. If “unnecessary” tests were requested, points would be deducted from the score. As the information was revealed, the differential diagnoses from each team would be refined, and ultimately a kidney biopsy would be interpreted to determine the histologic findings. The team with the most points would predict the biopsy findings and have the first chance to interpret the findings.
THE COMPETITORS:

TEAM PODOCYTE represented by nephrology fellows from Mt. Sinai, Stony Brook, Emory (Drs. Arun Kottarathara, Samira Farouk, Marianne Camargo, Martine Pollack-Zollman, Dilini Daswatta, Marc Saad)

TEAM TUBULE represented by Lehigh Valley, Cleveland Clinic, University Colorado Denver, University Missouri, University Alabama-Birmingham, Henry Ford Hospital (Drs. Krishna Komanduri, Arjun Sekar, Pratik Shah, Gurwant Kaur, Ewalola Ijaduola, Reddy Singasani)
THE CASE:
A 51-year-old Caucasian male was referred for evaluation of elevated serum creatinine level. His past medical history includes hypertension, hypothyroidism, and monoclonal gammopathy of undetermined significance 9 years ago with an M-protein level of 4.36 g/L. He was hospitalized 5 weeks ago with worsening anemia and back pain, for which he was taking ibuprofen. His medications for his chronic conditions were was amlodipine, aspirin, and levothyroxine. He was diagnosed with multiple myeloma, had serum free light chains with a kappa/lambda ratio of 220 and started on chemotherapy with bortezomib, dexamethasone, and thalidomide. Over the next 2 weeks, his free light chain kappa/lambda ratio improved to 50, but his Cr began to rise from a baseline of 1.35 mg/dL to 2.5 mg/dL, which prompts a nephrology referral.
FIRST DIFFERENTIAL DIAGNOSIS DISCUSSION:
The initial differentials between the 2 teams at this point were relatively similar, both considering multiple myeloma related kidney diseases such as cast nephropathy, light chain deposition disease, amyloid, and also non-myeloma related diseases such as NSAID induced minimal change disease.
CASE CONTINUED:
Further information and testing at this point was determined by the competing teams, arguing for the utility of various serum and urine tests, imaging, and consults from other subspecialties.
BP 180/86, HR 80 bpm, Temp 98.4 degrees, RR 19, pulse ox 97% on room air. Exam reveals bilateral lower extremity pitting edema and a 3/6 systolic murmur at the right upper sternal border.
Urinalysis revealed a specific gravity of 1.010, pH 7.0, moderate blood, many RBCs, and >100 protein on dipstick. Quantification of the urine based on a spot urine protein:Cr ratio was 1.5 grams/gram. CBC trend revealed a Hb drifting from 9.2 to 7.5 g/dL, WBC count from 2.4 to 1.37K, and a platelet count trending down from 140 to 100K.
SECOND DIFFERENTIAL DIAGNOSIS DISCUSSION:
The differentials for both teams expanded at this point to also include thrombotic microangiopathy (TMA), and the fellows appropriately worked this up by requesting a peripheral smear which revealed schistocytes and LDH/haptoglobin levels which were consistent with hemolysis. ADAMTS13 activity was normal.
At this point, before a kidney biopsy was performed, Dr. Jhaveri asked the fellow teams what they suspected they might see histologically. Their responses included thrombi in the capillary loops and arterioles, possible glassy fractured casts in the tubules, and subendothelial deposits seen on electron microscopy (EM).
HISTOLOGIC DIAGNOSIS:
Red cell and fibrin thrombi were seen in the glomerular capillaries and arterioles on light microscopy in addition to endothelial injury with arterial intimal mucoid widening on light microscopy. Immunofluorescence was negative, and no electron dense deposits were seen on EM, although fibrin tactoids were identified (see this post from the Atlas of Renal Pathology for a comparable image).
So with a histologic diagnosis of TMA, the next step was to make the clinical diagnosis. What was causing this? Again, this sparked lively discussion ranging from atypical hemolytic uremic syndrome to myeloma related TMA.
FINAL DIAGNOSIS:
Ultimately, Dr. Jhaveri made the final diagnosis of “TMA likely related to bortezomib therapy” and gave some insight into recognizing this disease, in addition to the increasing prevalence of this pathophysiology in other proteasome inhibitors (see this editorial in regards to carfilzomib).
CONCLUSION:
This hour was a lively discussion that emphasized several advantages that this type of teaching can provide over traditional presentations. Working with other team members, pooling collective knowledge, “gentle” competition, and considerations for appropriateness of medical testing all played an important role in making the correct diagnosis while learning along the way. Similar formats can be developed by any fellowship programs and should be individualized for their institution and learner levels.
Thanks to Drs. Kenar Jhaveri, Hitesh Shah, and James Pullman for moderating this session, and to all of the wonderful nephrology fellows who participated!
Posted by Dr. Timothy Yau, M.D.
Washington University School of Medicine, Division of Nephrology, St. Louis, MO
Live from Chicago, Illinois at the 50th ASN, #KidneyWk 2016
The next part was actually so much more fun ! The nephrology challenge 🙂
Just about to post one on that session as well!
It’s a great idea to teach by leading people through a case, a little competition makes it even nicer . In Poland it’s sometimes done as a part of congreses od conferrences and it’ s always fun , making us remember more afterwards 😀
Thank you for this challenged activity and sent it in my email.My knowledge is challenged and my brain is warmed. Thank you.