
#NephMadness 2017: The Effluent Eight
The first round results had a number of upsets. The second round represents the regional champions. Did the Blue Ribbon Panel break your heart and your bracket? Tweet your reaction and score with hashtag: #Effluent8
Glomerulonephritis Region

Steroids for IgA entered the Saturated 16 on house money having upset Protocol Biopsy, but they were no match for Anti-PLA2r which looks like it is on a mission. This was a no-doubter from tip-off to the final buzzer.
Anti-PLA2r wins 8-1.
Comments from the BRP:
Something getting at pathogenesis and useful for diagnosis vs. continued empirical treatment.
Steroids for IgA make a desperation 3 at the buzzer (along with a no-call by the ref) to advance through the 1st round. Don’t expect they’ll have it against the big guns like Anti-PLA2r.
I Love lupus nephritis, I Love renal pathology, I Love paradigm shifts, and protocol biopsies in lupus would make me complete. I’m also so tired of treatments (non-treatments?) for IgA nephropathy. It is such a common disease and there have been some big steroid studies recently for proteinuric IgA, but with contradictory results, I am downright nihilistic about treatment with steroids. Still, the potential impact is so great I gave in and voted for IgA in that first round. Indeed, it advanced. Now: PLA2R Ab v rituximab for MCD. I Love (get used to that word…) rituximab for MCD, it has never failed me. But PLA2R Ab testing (histologic and serologic) is even cooler, more interesting, and going to change the way we diagnose and manage MGN. I picked it over rituximab and it also advanced, and I have to vote for it here again, as it is time for this nonsense of steroids for IgA to end. IgA just keeps dribbling out of bounds while PLA2R hits the big 3 pointer. I wonder how the rest of the Blue Ribbon Panel will vote? Great job, Tim Yau and Bea Concepcion (2 of my former fellows!), as well as Michelle Rheault, on the discussion and visual abstracts for this section!
Steroids for IgA in the Effluent Eight? Would be a travesty.
History Of Nephrology Region
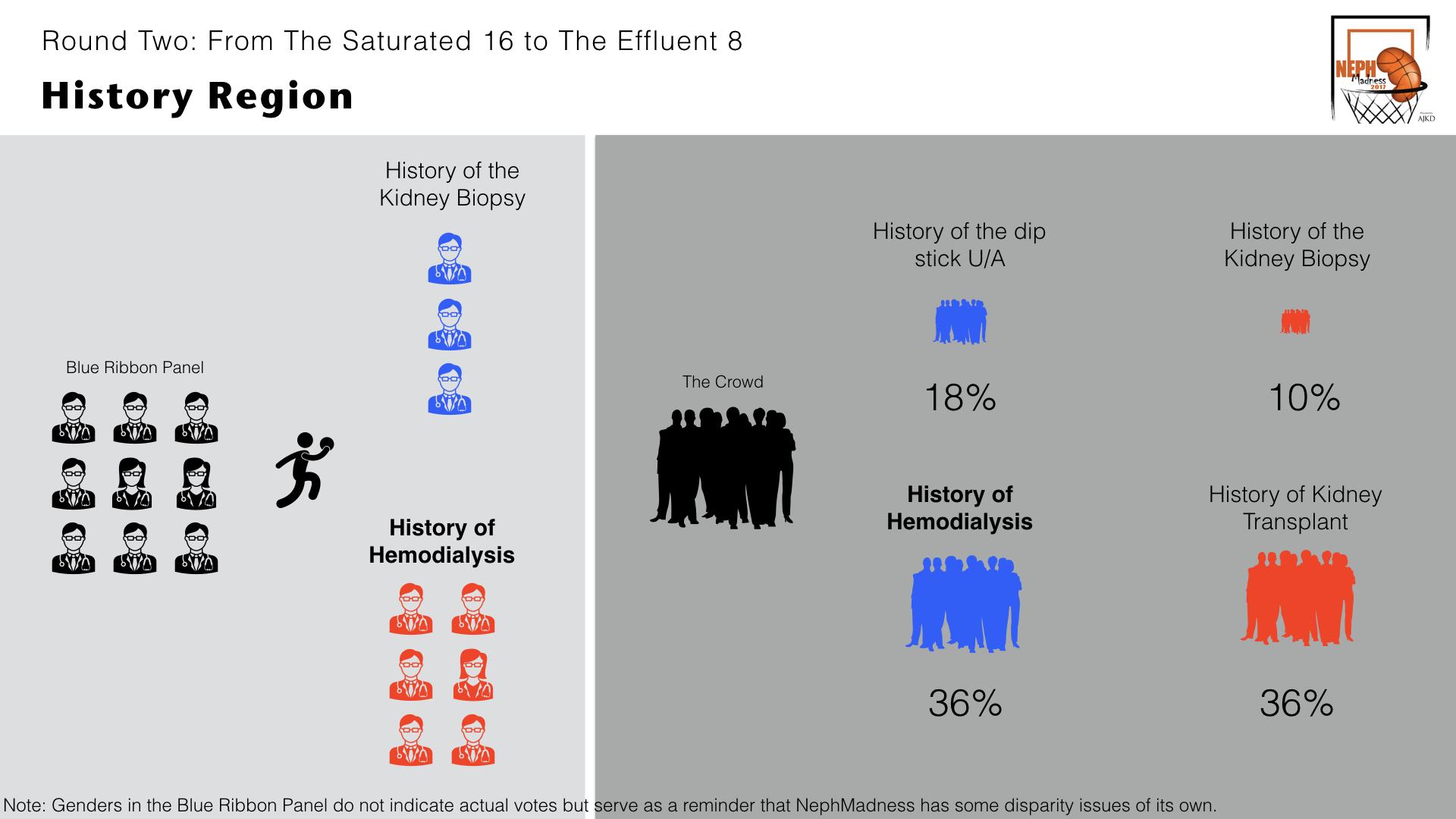
History of Hemodialysis may be the darling of the tournament. Even far away from home it felt like a home game with the crowd solidly behind ol’ hemo. Despite that, History of the Kidney Biopsy played tough and it was still close going into the final minutes, but Coach Kolff ran his infamous Sausage Casing around the Washtub pic play and it was all over.
History of Hemodialysis wins 6-3.
Comments from the BRP:
Diagnosis vs treatment. The story of hemodialysis is too compelling.
Round 1: hx of renal biopsy vs hx of urinalysis: Both histories were amazingly well-researched and written (amazing, Paul Phelan!). Renal histology is so much fun when you get good at it, and while the U/A can be so clinically important it is also kinda boring. Biopsies are a slam dunk alley-oop, while the urinalysis a free throw. You do get a lot more points with free throws. But if you remember the narrative on this topic it had a picture of Dr. Robert Kark. Dr. Kark was from my institution, Rush, who occasionally came to biopsy conference when I was a fellow. He was a sweet man with the nickname of “Googoo” (only Dr. Edmund Lewis would/could call him that). Dr. Kark, a gentle soft-spoken man, would refer to minimal change disease as “asthma of the kidney” in his South African accent… how great was that? What an honor to have even met him. He and Robert Muehrcke, Victor Pollack. and Conrad Pirani essentially defined histologic lupus nephritis! I HAD to vote for the renal biopsy. Somehow, and I am shocked, it beat Urinalysis! History of HD vs Tx. The histories of both tell the stories of an amazing collection of problem-solvers, outside-the-box thinkers, innovators, humanitarians. How do you pick one over the other? Both therapies prolong lives, improve quality of life, are amazing translations of technical and biologic advancements. I picked HD because it simply impacts more people. Can you imagine if we did not have hemodialysis? HD did beat Tx. And as emotionally attached I am to the history of the renal biopsy, there is no way it wins over HD. I will be shocked if HD doesn’t advance further.
Making Nils Alwall proud. (Kurkus et al, AJKD 2007)
Dialysis Region

People were still shaking their heads in disbelief over Kt/V urea‘s improbable victory over Depression in Dialysis at tip-off for the second round game versus Patient-Reported Outcomes. Patient Reported Outcomes did not seem surprised or put out by the unexpected opponent and dominated the boards, out-rebounding Kt/V urea 17 to 6. The second chance points made all the difference as PRO cruised to comfortable victory.
Patient Reported Outcomes wins 7-2.
Comments from the panel:
PRO vs. a calculation of modest usefulness?
Kt/V Urea has had a good long run, but the field is advancing without them.
The next round paired KT/V v Depression in HD. Depression in HD is just the tip of the iceberg, this topic is NOT going away. It would have won against many other topics, but it was paired against KT/V urea and this was such a great discussion by Nikil Shah about the concept of adequacy (inadequacy), how to measure, and what to measure that even though KT/V urea is so very flawed, this topic is of paramount importance, I picked it and it did beat Depression. Neurocognitive declines in HD v Patient Reported Outcomes. I voted for Neurocognitive as this is a big deal for patients that is so underappreciated, and is yet another indication of the inadequacy of HD. It lost to Patient-reported outcomes – I’ll bet this one was close. Not picking Patient-reported outcomes the first round, and how I feel about KT/V urea, I am advancing KT/V urea for this second round. I will be surprised if it also does not advance.
Biomedical Research Region

Both heavy favorites came out of their first round games with momentum. But the hype machine surrounding CRISPR-Cas9 seemed to get in the heads of the Gene Microarray players and they folded like a cheap suit.
CRISPR-Cas9 wins 8-1.
Comments from the BRP:
CRISPR is just beginning to explore it potential. They have speed, size, bench depth, and a really good coach. For a top early-round match-up, this should be the game to see.
This next grouping Biomedical Research was a struggle for me as I am no basic scientist, and even with the excellent descriptions by Matt Sparks, my head was spinning. I felt like a Neanderthal reading that section. But I’ll keep this simple: Can you imagine anything cooler, sexier than CRISPR-Cas9? It has to be “the picket fence” of Biomedical Research (from “Hoosiers,” the best basketball movie ever? Watch it again if you haven’t seen it recently). It won. Gene microarray v Two-Photon Microscopy: I picked Gene microarray because it had a lot more fancier words in the description than its opponent, sorry… It also won, go figure. But this round has to go to CRISPR-Cas9. I only hope they advance this soon so it can splice (“edit”) me some new genes. No doubt I am loaded with mutations. Diaper dandy!
Disparities in Nephrology Region

Genes in ESKD Disparity riding on their senior guard, APOL1 was unflappable despite the aggressive play of System Factors in Transplant Disparity. The teams were even through most of the match but APOL1 stole an inbound pass and converted a layup to ice the victory. Win and move on for Genes in ESKD disparity.
Genes in ESKD Disparity wins 5-4.
Comments from the BRP:
System factors we may be able to address; Genes, not so much.
System Factors in Transplant Disparity could win this, but this is a young team that will have trouble going much further.
Disparities, what a clever section. Major Kudos to Matt and Joel (et al) who came up with all these sections. Genes in ESKD v Society in ESKD. Silvi and Swapnil took a very difficult subject and made a real case for each of these! I picked Genes, but it was close and I think it was the amazing story of APOL1, one I can never get enough of (Headline: “Evolutionary trypanosomal protection backfires in modern world”) that decided it for me. Genes did win. Pt factors in Tx disparity v System factors in Tx disparity. This was easier for me as we have the opportunity to do more with the System than the patient. We are the System, we have control over our part, and we frequently “double dribble” on that. Picking between Genes and System, I have to go with Genes. The racial (genes) disparity in kidney disease is overwhelming.
Transplant navigators anyone?
Genetics Region

The best thing that ever happened to the Podocytopathies was changing their mascot from the glomerular epithelial cell to the podocyte. All of a sudden it became everyone’s favorite renal tissue. Genius. While licking their wounds from the shelacking they received, the Zebrafish are changing their name to a more carnivorous sounding fish, maybe the Terminator Fish?
Podocytopathies wins 7-2.
Comments from the BRP:
Although a zebrafish with a podocytopathy might go all the way
Podocytopathies has beautiful ball handling, from genes to proteins to structure. A joy to watch.
Podocytopathies v ciliopathies. I picked cilia, but podocytes won. I was surprised. Cilia diseases are more interesting, and there aren’t 6,000 letter mutations for 6,000 different causes of FSGS that I will never memorize. And just getting rid of the term nephronophthisis (a word I have never successfully pronounced) is enough to make this topic a winner for me. The podocyte is a bounce pass, the cilia a swish, nothing but net. But not for my fellow Blue Ribbon Panel members. I bow to their wisdom. Fruit fly vs zebra fish. I have such wonderful memories of learning Mendelian genetics using fruit flies as an undergrad. But Arthropod v Fish. Homer Smith wrote “From Fish to Philosopher” (a must-read for any student of nephrology), not “From Insect to Philosopher.” I picked my oceanic ancestor and it won. Podocytes v a transparent fish. While I’m not optimistic that we will ever do anything more than find a lot of mutations that affect the podocyte, there are a lot of people with podocyte diseases, and I think the future is strong for this field, so I now have to give the podocyte its due respect. Podocytopathies it is! Great job, Brian Stotter. And how in the world did Cathy Quinlan do those amazing videos? For Best Animated Short, the Oscar goes to…
Diabetic Nephropathy Region

This was the marque match up of the second round. Two therapeutic heavy weights. ACEi and ARB comes to the tournament backed by dozens of RCTS and decades of experience. The SGLT2 Inhibitors, a newcomer, came with a single, powerful study, promising a huge benefit. Riding the momentum of EMPA-Reg, the SGLT2i overcame the champs.
SGLT2 Inhibitors win 6-3.
Comments from the panel:
New stuff vs. old stuff. Easy.
SGLT2 doesn’t have the guns to run with the big guys – ACEi/ARB win this going away.
Anna Burgner nicely presents a balanced view of an unbalanced topic. ACEi and ARB for renoprotection v glycemic control in DN. At least for renal disease this is like Michael Jordan (ACEi/ARB) playing me (Glycemia), one-on-one. I was involved in the Captopril and IDNT trials. Human “renoprotection” was first demonstrated from the captopril trial. I eat and breathe RAAS inhibition. Glycemia didn’t have a chance. SGLT2 inhibitors v GLP1 Antagonists. Who even thinks of developing a drug to spill glucose? I still can’t get over that. It is akin to adding a shot clock to NCAA basketball, in that there was a time when there was no shot clock! The fact that studies on SGLT2 inhibitors had positive renal secondary endpoints is like making the second free throw of a “one and one”. GLP1 antagonism is close, but bounces off the rim. SGLT2 vs ACEi/ARB. This is tough. The new kid SGLT2 is wearing Air Jordans, ACEi/ARB is wearing Converse All Stars (you have to be old to get that reference). I ran into a patient last month from the Captopril study (early 1990s) who I told would be on dialysis in 3-5 years. Her creatinine is 1.4 twenty-five years later! At least for now I have to stick with ACEi/ARB.The Duke of this field – good every year.
Nutrition Region

The Feeding During Dialysis team came into this team completely outgunned. The Microbiome and the Kidney looks like a juggernaut with a 7-foot center and forward with ball handling skills. Team Microbiome is looking like it has the legs to go deep in the tournament.
Microbiome and the Kidney wins 7-2.
Comments from the panel:
Microbiome looks like the class of this Division.
Protein restriction v Feeding during dialysis. The early models of CKD progression involved rat 5/6 nephrectomy developing hyperfiltration FSGS associated with glomerulomegaly and glomerular HTN. Two things prevented it: protein restriction and ACEi. Both lowered glomerular capillary pressure, prevented glomerular hypertrophy, proteinuria, and FSGS. Protein restriction worked on the afferent arteriole and ACEi on the efferent arteriole. ACEi was translated to humans in the Captopril trial, and protein restriction should have been confirmed by the MDRD. The Captopril Trial was a huge success while the MDRD was a negative trial, but I still believe protein restriction probably has a renoprotective effect. However, which would you rather do, take a pill or radically change your diet? Perhaps they work better together (unanswered). Regardless, RAAS blockade took off and protein restriction withered. Feeding on dialysis has two sides, but the nutrition data is compelling. Sitting 4 hours for HD is torture enough, and we typically limit so much during it. How ironic it would be if eating is actually better for them. I like this topic! I picked eating as did the Blue Ribbon Panel. Microbiome v Omega 3 fatty acids. The microbiome alone is such an amazing thing by itself (10 times more bacteria than cells in our body), then throw in uremic toxins, real uremic toxins made there, and you have a very cool topic. The microbiome is every seat in the stadium filled with supporting fans, while the body is only the team and its bench. Omega 3: BORING. So is it microbiome or feeding on HD? I love the concept of non-urea uremic toxins, it has got to be the biome. The team of Joel and Swapnil remind me of Michael and Scottie for this section.
It’s like Gatorade – but with protein.
Ladies and Gentlemen, we present your Effluent Eight!

Filtered 4 will be announced on Friday, March 31!
![]()
Leave a Reply