
#NephMadness 2019: Plasma Exchange Region
Submit your picks! | NephMadness 2019 | #NephMadness | #PLEXRegion
Selection Committee Member: Andre Kaplan
Andre Kaplan is Professor of Medicine and Chief of Blood Purification at UConn Health and is currently President-Elect of the International Society for Apheresis (ISFA). For the last 35 years, he has been involved with the clinical and laboratory evaluation of numerous blood purification techniques.
Writer: Paul Phelan @paulphel
Paul Phelan is an academic clinician at the Royal Infirmary of Edinburgh, Scotland, where he serves as a Consultant Nephrologist and Renal Transplant Physician. He is an honorary senior lecturer at the University of Edinburgh and a Fellow of the Royal College of Physicians of Edinburgh. His research interests are focused on renal genetics.
Competitors for the Plasma Exchange Region
ANCA Vasculitis vs Light Chains
Pre-Transplantation vs Post-Transplantation
Plasmapheresis has history in NephMadness. It has been a bit-part player for several teams including in last year’s Transplantation Region but 2019 sees it gets a region of its own.

Copyright: umarazak / Shutterstock
Plasmapheresis, simply removal of plasma, or as it’s currently performed, therapeutic plasma exchange (TPE), is used for a myriad of diseases, a large proportion being in the realm of the nephrologist. Potential renal indications for therapeutic plasma exchange (TPE) include:
- Anti-GBM disease
- Pauci-immune rapidly progressive glomerulonephritis (usually ANCA associated)
- Focal segmental glomerulosclerosis (recurrence post-transplant)
- IgA nephropathy/Henoch Schonlein Purpura (rapidly progressive)
- Transplantation (anti-HLA, anti-A, anti-B antibodies)
- Hemolytic Uremic Syndrome / Thrombotic Thrombocytopenic Purpura
- Cryoglobulinemia
- Multiple myeloma (cast nephropathy)
- Antiphospholipid syndrome
A patient with multiple myeloma with life-threatening increased plasma viscosity was the earliest description of plasmapheresis (1952). TPE is most commonly performed using centrifugation devices used in blood banking procedures, which also allows selective cell removal, such as leukapheresis. However, TPE may also be handled by nephrologists employing hemodialysis equipment using a plasma-cell separator in place of the hemofilter. TPE is warranted to remove a pathologic substance, such as an antibody, light chain, cryoglobulin, immune complex, or endotoxin that is too large to be removed by high flux hemodialysis (say, molecular weight >15 kDa; note IgG = 150 kDa) and have too long a half-life so that waiting for endogenous clearance is not desirable (see image below for kinetics of IgG removal with TPE). TPE also involves replacement of fresh plasma which may be advantageous in certain conditions (eg Thrombotic Thrombocytopenic Purpura) by replenishing ADAMTS13 as well as removing von Willebrand factor multimers and ADAMTS13 autoantibodies. Check out this excellent Core Curriculum from our selection committee member, Dr. Andre Kaplan.

Progressive decrease in immunoglobulin G (IgG) levels after 3 consecutive therapeutic plasma exchange (TPE) treatments equaling 1 plasma volume each. Intertreatment increases between treatments represent a combination of extravascular to intravascular reequilibration and a variable amount of new IgG synthesis. Adapted from Kaplan, © Andre Kaplan.
TPE for ANCA-Associated Vasculitis (AAV)

Figure 2 from Fogo et al, AJKD, © National Kidney Foundation.
NephMadness loves controversy and TPE for AAV (we’re sticking with this name!) certainly arrives into the 2019 tournament on the back of a storm of opinions. It wasn’t always like this. Up until recently we all knew exactly when and when not to use TPE in AVV, right? However, the waters have been well and truly muddied since then. It’s reasonably well-accepted that MPO-ANCA & PR3-ANCA are pathogenic in these diseases so it makes intuitive sense that removing them will help.
Evidence for ANCA pathogenicity comes from:
- Animal models: T & B cell deficient mice & MPO-knockout mice injected with anti-MPO develop a pauci-immune glomerulonephritis.
- Famous case report of placental transmission of anti-MPO resulting in transient neonatal pulmonary-renal syndrome.
- There’s also this circumstantial evidence; large GWAS (certainly for such a rare disease) demonstrating that patients with ANCA-MPO & PR3-ANCA segregate genetically. Moreover, polymorphisms in the gene encoding proteinase 3 were associated with PR3-ANCA.
Indications for TPE in this disease have traditionally been:
- Severe renal disease: on dialysis or severe renal dysfunction
- Pulmonary hemorrhage
- ‘Double positive disease’- co-existent anti-GBM autoantibody. These patients tend to behave like anti-GBM disease, the poster child of renal indications of TPE (despite a paucity of robust data supporting its use).
TPE is generally recommended for severe alveolar hemorrhage (although without much evidence). In patients without severe lung involvement, it has gained a role in attempting to prevent end-stage kidney disease( ESKD) in patients with severe renal disease at presentation, due largely to the MEPEX trial. MEPEX (n=137) included patients who had a serum creatinine > 500 µmol/L (5.8 mg/dL) or requiring dialysis at presentation. Patients were randomized to seven TPE treatments or IV methylprednisolone (should both groups have received the same induction steroid?), with both groups then receiving oral steroids and cyclophosphamide. At one year, TPE was associated with a risk reduction of ESKD of 24% and similar severe adverse events and patient survival. Based largely on these data, TPE became standard of care for severe renal disease in AAV. A follow-up to MEPEX, which appeared to attract much less fanfare, had almost 4 years data and demonstrated no significant difference between the groups for a composite of death & ESKD.

Adapted from Walsh et al, KI © International Society of Nephrology.
How should we interpret this study? Our selection expert argues that a one year benefit of 24% risk reduction in ESKD is not something to scoff at. According to the most recent USRDS, one year of hemodialysis costs $90,000, while six TPE treatments cost around $12,000. Thus, even ignoring the fact that most patients would rather not be on dialysis, if only 14% of patients treated with 6 TPE treatments avoided dialysis for at least one year (and the results of MEPEX are considerably better—with 43% on dialysis at 12 months without PLEX and only 19% on dialysis in 12 months with PLEX), it would be financially better for society to offer six TPE treatments to all those with aggressive AAV induced GN. To sum it all up, if six TPE treatments can help some patients avoid dialysis for as little as one year, that is a fantastic outcome which may be well worth the effort.

Visual Abstract by @madmagicdoc on Jayne et al
It is also possible that a beneficial effect of TPE in preventing ESKD exists in cases of AAV earlier in their natural history before significant scarring has occurred. This was perhaps supported by this meta-analysis which demonstrated a benefit with TPE in patients with a broad spectrum of renal function at presentation. The authors were careful, however, to point out that due to the size and quality of the included trials, there was insufficient evidence to reliably determine if TPE reduces the composite of ESKD or death.
Next came the star player on the team, the largest trial ever conducted in AAV. PEXIVAS hasn’t quite arrived just yet, but did make an entrance via an oral presentation at #ERAEDTA18 in Copenhagen. PEXIVAS was a 2×2 factorial trial with the 2 strategies being TPE (yes/no) and steroid dose (standard/low dose). Overall, 700 patients with severe disease, defined as eGFR <50 ml/min or pulmonary hemorrhage, were randomized, with the TPE group receiving 7 exchanges within 14 days. All patients received cyclophosphamide or rituximab and initial pulsed methylprednisolone (unlike MEPEX, this was standardized for both groups). Median creatinine was ~330 umol/L (3.8 mg/dL), ~20% needed dialysis, and 27% had any lung hemorrhage (9% classed as severe).
Overall results apparently demonstrate no difference in the primary endpoint, a composite of death and ESKD, with or without TPE. Secondary endpoints of the individual primary endpoint as well a sustained remission were also identical. It’s fair to say that PEXIVAS has caused quite a stir (see early Twitter chat), and at the time of this writing, it’s not even published yet. Closely studying the Kaplan-Meier curve, it could be said that there appears to be a benefit to TPE in the first year, which is subsequently lost. Some commentators have argued that there may be subgroups that would benefit from TPE (most severe disease, florid pulmonary hemorrhage?).
It should be noted that PEXIVAS patients had lower serum creatinine values than MEPEX. Teasing out if pathological lesions correlate with treatment outcomes will be interesting. Either way, it’s hard to argue with the overall result appearing to show no benefit with TPE. I still see lots of TPE being performed in AAV so we will need to wait and see how practice-changing this trial becomes.

Adapted from @ERAEDTA tweet.
At this point, the place of TPE in the treatment of AAV to me is unclear with confidence in its use being eroded with long-term of follow-up of MEPEX and now PEXIVAS. PEXIVAS is a fantastic effort with a huge number of patients recruited considering the rarity of the disease. Exploring subgroups of this rare disease that may benefit from individual treatment will be a real challenge and this trial may be as good as it gets, at least for the foreseeable future. Why is there that early benefit in the plasma exchange group? The curves merge later on, but is the ESRD benefit in that first year something to consider (as we explained and saw in MEPEX, buying a year or two off dialysis is a huge potential benefit)? The hypothesis for removal of pathogenic ANCA antibodies make sense but the data leaves us back at square one.
Light Chains
There are a myriad of renal manifestations of multiple myeloma, largely due to secreted toxic free light chains (FLC). AKI due to cast nephropathy (myeloma kidney) is among the most severe. It is associated with a worse prognosis, often leads to irreversible renal injury and ESKD, and is therefore an indication for urgent treatment. As mentioned in the introduction to this region, removal of nephrotoxic FLC in myeloma cast nephropathy has long been considered an attractive strategy, even before precise pathogenesis of the renal injury was understood.

Copyright: alexander h. schulz / Shutterstock
However, this approach has not been established and remains controversial. As FLC are small proteins, they are present in similar concentrations in serum, the extravascular compartment, and any 3rd space fluid. Even a single TPE treatment may remove 2/3 of the intravascular FLC, and most proponents of TPE for light chain removal recommend 5-7 treatments over 7-10 days. Our earliest data come from a small randomized Italian study in 1988 which suggested a benefit for renal recovery by adding TPE to standard treatment. Our second trial was a multi-center trial from Canada, which suggested a benefit for TPE (dialysis dependent at 6 months: 26.9% without PLEX vs. only 12.8% with PLEX) but was underpowered and did not show conclusive benefit. Although this was the largest trial of TPE for cast nephropathy, there were criticisms regarding lack of confirmatory renal histology or measurements of serum FLC. The elephant in the dressing room for this team is high cut-off hemodialysis (HCO-HD), a player who has recently become a bitter rival to TPE for treatment of myeloma kidney (more on that below).
Despite uncertainty regarding the merits of TPE for cast nephropathy, it continues to be used by many clinicians. A typical TPE regimen is 5-7 exchanges within the initial 10 days; however, this may be guided by FLC burden. There is evidence that reducing serum FLC by 50-60% is associated with a favorable renal outcome. It should be noted that this study comprised 2 cohorts, one from Rochester that used TPE to reduce serum FLC and another from Birmingham, UK, that used extended (6-8 hour treatments) HCO-HD. There was significantly more renal recovery for dialysis-dependent patients in the HCO-HD group (although no difference in the groups overall). Hutchison et al, co-authors of the above study, had previously developed a compartmental model for AKI due to cast nephropathy including initial FLC concentrations, clearance rates, half-lives, production rates, volume of distribution and equilibration between intravascular and extravascular compartments, and tumor killing rates. It is worth noting that the model has serious flaws. It indicates that plasma exchange would remove only 25% of the total amount during a 3-week period but that extended HCO-HD may remove 90% of FLC during the same window. Keep in mind here that piddly doses of plasma exchange were compared to 10+ hours of HCO-HD with 2-3 filters in series, so we’re comparing the height of Mugsy Bogues to Manute Bol.
HCO-HD uses dialyzers with membranes containing a large pore size, up to 50 kDa (for comparison high flux HD pore size approximately 15 kDa; kappa light chain molecular weight 22.5 kDa, lambda 45 kDa). Encouraging case series suggest that extended HCO-HD effectively drops serum FLC levels and associates with enhanced renal recovery. Protocols are aggressive, employing initial daily 8-hour sessions in an effort to remove more FLC, necessitating albumin and phosphorus replacement. This theory has been tested in 2 RCTs. EuLITE started recruiting in 2008, apparently completed in 2014, and curiously is still not published, although results were presented at UK Kidney Week & the European Haematology Association in 2016 (n=90). These demonstrated no improvement in renal recovery, no difference in FLC levels, and increased mortality and a high infectious burden with long and repeated treatments of HCO-HD.
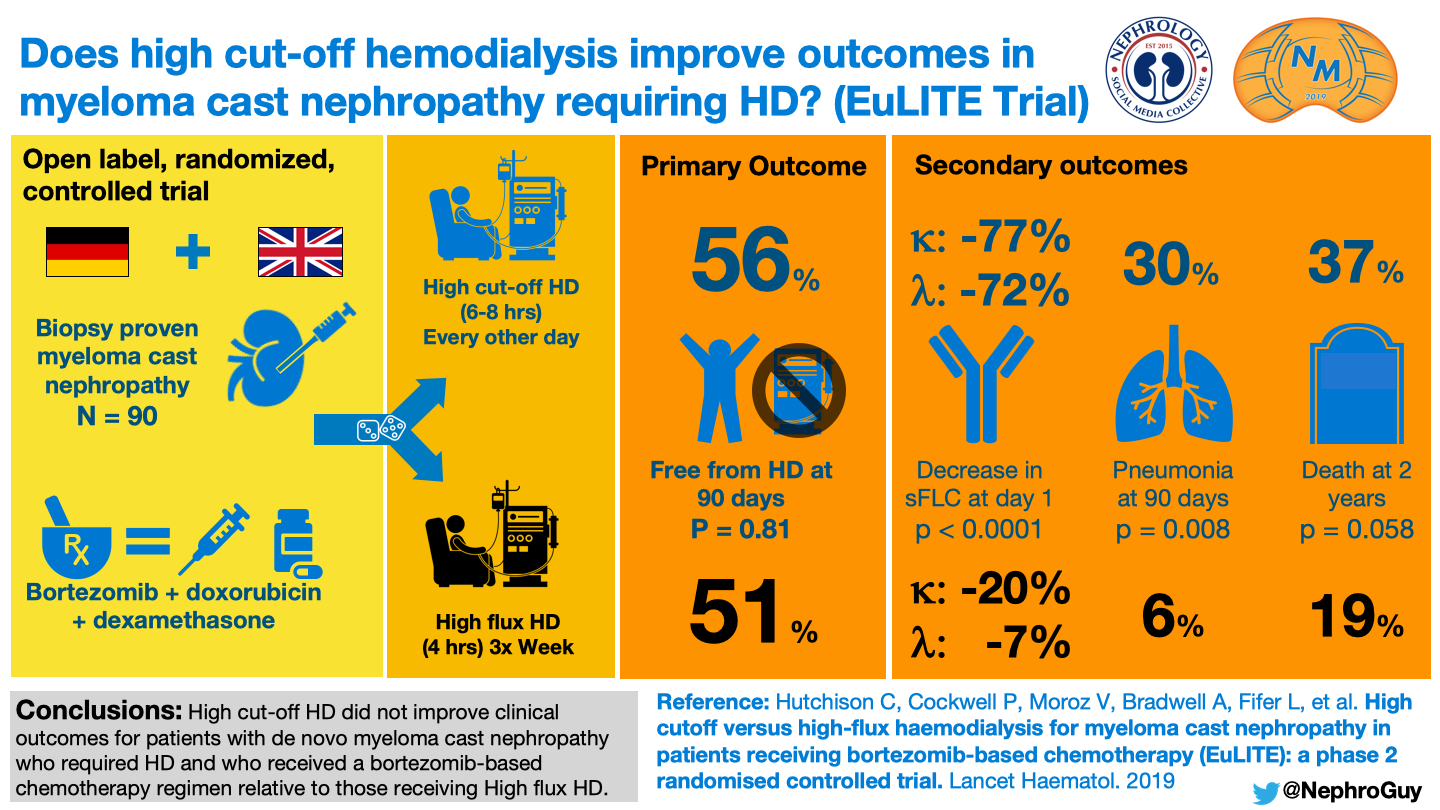
Visual Abstract by @NephroGuy on Hutchison et al
The second study is MYRE (n=98), a trial conducted in France and published in JAMA and covered by NephJC. They randomized patients with cast nephropathy needing dialysis to HCO-HD or conventional high-flux HD with all patients receiving early bortezomib-based chemotherapy. The primary endpoint was dialysis independence at 3 months which was not different (41.3% in high-HCO-HD group vs 33.3%) although the secondary endpoints of dialysis independence at 6 & 12 months were significantly improved with HCO-HD (56.5% vs 35.4% at 6 months; 60.9% vs 37.5% at 12 months).
It is not immediately clear what this means and how early HCO-HD would translate into more renal recovery at 6 months but not at 3 months, although one could conclude that it takes time to reverse the tubular and interstitial damage associated with light chains even if their removal was enhanced. In my opinion, these tantalizing results do not shut the door completely on the use of HCO-HD in multiple myeloma. It was a strange experience reading MYRE, a trial actually published, on the back of knowing the disappointing top-line results from EuLITE. It’s impossible to marry the somewhat conflicting results of the 2 studies, without seeing the full data, and I wonder if MYRE would have been received more positively by the community (myself included), if we hadn’t previously been deflated by EuLITE, despite us not having a manuscript to read.

Visual Abstract by @edgarvlermamd on Bridoux et al
The critical intervention for patients with myeloma cast nephropathy remains early initiation of effective chemotherapy, no matter what attempts are made at enhancing FLC depletion. The introduction of bortezomib-based regimes has coincided with markedly improved outcomes for these patients. Removal of FLC by any extracorporeal method is doomed to failure, regardless if any true benefit of light chain removal exists, if a brisk early reduction in light chain producing plasma cells does not occur.

Adapted from Bridoux et al, JAMA, © American Medical Association
Pre-Transplantation
TPE for incompatible transplantation is a team of its own this year having been a peripheral figure in previous tournaments (see NephMadness 2017 Transplantation Region for further reading). It plays with a direct approach but is crudely effective against its opposition. Natural rivalries exist with ABO -incompatible (ABOi) transplantation, HLA-incompatible (HLAi) transplantation, and antibody-mediated rejection (ABMR). The use of TPE to broaden access to transplantation for patients with incompatible donors has opened up transplantation as an option for many ABOi pairs and certain HLAi pairs. This year’s scouting report will concentrate on TPE rather than incompatible transplants in general.
Copyright: kerale / Shutterstock
Let’s start with some history, which is always popular in NephMadness. The potential merits of TPE were demonstrated in 1970 by Thomas Starzl’s group who described ‘successful’ outcomes in transplanting porcine xenografts into dogs, with success defined as prolonging graft survival to >100 minutes. Transplant physicians were already aware of plasmapheresis techniques to prepare emerging anti-lymphocyte globulin preparations from sheep and horses, which were proving extremely valuable in salvaging organs from rejection. A potential use of TPE to facilitate ABOi transplantation was soon recognized.
ABOi Transplantation
As well as being present on red cell membranes, ABO blood group antigens are also expressed on various other tissues including vascular endothelium and renal tubular cells. This leads to ABMR following ABOi transplantation due to naturally occurring anti-A/B antibodies. An early report of ABOi transplantation from amongst the first ever transplants in Boston describes a case of primary non-function in a B donor to O recipient. To put this paper into historical context, the cited literature in this report includes Carrel’s descriptions of transplanting kidneys in cats and dogs in the early 1900s!
Depending on population prevalence of ABO blood groups, there is a 30-40% chance that any 2 individuals will be ABO-incompatible. Reversal of ABMR after inadvertent ABOi kidney transplantation was demonstrated in 1982, which paved the way for planned living donor procedures. Modern, safe ABOi transplantation was subsequently pioneered in Japan and later embraced worldwide with TPE being the cornerstone of therapy, by removing pathogenic antibodies, to enable these transplants to proceed safely. The number of TPE sessions needed depends on the initial antibody titer with transplantation recommended to occur as soon as possible after achieving adequate desensitization.
Due to a lack of randomized trials in this area, many uncertainties remain:
- What goal titer should be aimed for (1:4 – 1:16 depending on the center)?
- Are different titers needed for A1, A2, and B antibodies? (we do know that rejection risk is different for these transplants – A1>B>A2)
- Is rituximab necessary? As mentioned in last year’s Transplantation Region, a tiered approach with omission of rituximab for low-risk cases may be safe.
- Is IVIg necessary post-TPE to downregulate new antibody production? We don’t use IVIg in Edinburgh, although we do perform TPE to a conservative titer of not more than 1:4.
- Is additional TPE necessary post-transplantation for an isolated rebound in antibody titer (in the absence of ABMR)?
This team has also recruited an exciting foreign competitor named immunoadsorption (IA) that has played mostly in the European leagues. This method allows for antigen-specific selective antibody removal, in this case anti-A and/or anti-B antibodies, achieved using carbohydrate columns with embedded A or B antigens. This should avoid adverse effects of TPE associated with non-selective removal of clotting factors and other important plasma components. Predictable, there is a lack of robust head-to-head data for TPE versus IA in this setting, although IA appears to achieve adequate A/B desensitization and is another option for transplant nephrologists that have access to this resource.
HLAi Transplantation
TPE is also widely employed for desensitization to enable HLAi transplantation. Generally, the aim is to render the cross-match negative prior to live donor transplant and then monitor closely for rebound alloantibody and subsequent ABMR, where immediate reinstitution of TPE would again have a major role. For anti-HLA desensitization, while it makes intuitive sense to perform TPE, there is a dearth of robust data supporting its use. TPE use was associated with better outcomes (more negative cross-matches and less ABMR) in this series form the Mayo Clinic: although the 2 TPE arms also included rituximab, one TPE arm also included anti-thymocyte globulin (ATG), and several patients underwent splenectomy compared to the comparator (who received high-dose IVIg). For more on HLAi transplantation in general, see last years NephMadness content.
Several small studies have reported the successful reversal of early ABMR in sensitized kidney transplant recipients using TPE, generally along with IVIg administration. The latter study used historical comparisons of high dose IVIg versus a combination low dose IVIg/TPE and rituximab for treatment of early ABMR, with the combination group having better outcomes. Again, given the heterogeneity of the regimes, was it the TPE or rituximab or something else that led to improved outcomes? These data have led to TPE/IVIg becoming standard of care of ABMR management with common regimens including 5-7 exchanges over a 10-14 day period.
There are trials planned to assess if additional treatments, including one using bortezomib, offer added benefit to TPE-based treatment. Unfortunately, for late/chronic ABMR, no interventions (including those employing TPE) have been shown to have any clinical benefit. IA may be an alternative to TPE in the treatment of ABMR, too, with this tiny randomized trial (n=10) reporting good outcomes in those receiving immediate IA, compared to those who only received IA as rescue therapy weeks later.
TPE is a crucial tool for transplant physicians for a variety of conditions, although like much of transplant medicine, what we do is not based on hard evidence and many uncertainties remain regarding optimal protocols and precise indications. Will this headline team live up to its stellar reputation when put to the test?
Post-Transplantation
Copyright: oatawa / Shutterstock
Recurrence of primary disease post-kidney transplantation is a problem we face across of spectrum of diseases, usually glomerular disorders. It is often difficult to predict who is at risk of recurrence and although TPE in certain circumstances and specific diseases may make sense, we often do it based on little evidence to guide us.
Recurrent atypical Hemolytic Uremic Syndrome (aHUS)
HUS that is not due to Shiga toxin-producing bacteria is predominantly caused by genetic abnormalities in the alternative complement system, usually with superimposed additional hits needed to trigger disease. These ‘hits’ may include infections, pregnancy, surgery (including transplantation), and malignancy. The introduction of eculizumab has been a game-changer for aHUS, which was traditionally treated using TPE; however, the well-documented exorbitant price of this agent may preclude its use in many health systems. In such circumstances, TPE would remain the mainstay of treatment for most genetic causes. aHUS often recurs post transplantation, particularly when the mutation is in a gene encoding the plasma proteins, complement factor H or factor I (CFH/CFI). This is in contrast to mutations in the gene encoding membrane cofactor protein (MCP), where recurrence rates are much lower (see table here for a selection of the most common gene mutations). It makes sense that genetic mutations in circulating proteins lead to higher rates of recurrence compared to mutations in genes coding for proteins located on the native renal endothelium. Recurrent aHUS is a clinically devastating complication, usually resulting in allograft failure.
Prophylactic eculizumab, when available, has also generally replaced TPE when transplanting individuals at high risk of recurrent aHUS. Moreover TPE will remove eculizumab if it’s been recently administered. However, if eculizumab is not available, aggressive early TPE may have a beneficial role.
As post-transplant HUS/thrombotic microangiopathy is frequently multifactorial in etiology, it makes sense to strictly manage patients at risk of recurrent disease to mitigate chances of TMA in the allograft. This may include aggressive blood pressure control, minimization of calcineurin inhibitors, selection of allografts with a low risk of ischemia reperfusion injury, and so on. This approach was elegantly (bravely?) illustrated by a group from the Netherlands who described 17 patients at high risk for recurrent aHUS who did not receive pre-emptive eculizumab, or TPE, but otherwise received scrupulous care to minimize endothelial insults. Only 1 patient developed recurrence after a median follow up of 25 months (my expanded thoughts on this study are here).
Recurrent FSGS
Using TPE for recurrent focal segmental glomerulosclerosis (FSGS) is widely accepted as a good thing to do despite a real lack of understanding as to how this may help and if it does help. Early recurrence of nephrotic syndrome is presumed to be due to a yet unknown ‘circulating factor’, with suPAR being a candidate, although confirming a direct causal role for suPAR in FSGS has proven controversial. Recurrent nephrosis may occur immediately with patients displaying heavy proteinuria by the end of the first post-transplant day. Predicting who will get early recurrence is challenging, largely because a focal sclerosis pattern of injury may have a broad range of underlying etiologies so it is often unclear if a patient has ‘circulating factor’ FSGS or not.
Risk factors for recurrence are variable and sometimes contradictory depending on the series you read but often include initial childhood presentation with rapid progression, white race, and recurrence in a previous allograft. Some series have mentioned receipt of a living related donor kidney as being a risk factor, although this is not consistent across the literature and in my opinion should not be a reason to preclude living donation in this setting. However, the donor-recipient pair should be counseled on recurrence risk.
Data from the UK demonstrate that initial steroid sensitivity (especially those achieving a complete remission) is a risk for recurrence. A series from Duke shows that familial FSGS, which is generally due to mutations in genes encoding podocyte slit diaphragm/actin cytoskeleton proteins, confers a very low risk of recurrence, which makes intuitive sense. Despite these data, early recurrent FSGS can often catch us unaware, especially if the primary renal disease was unclear or if it occurs in an adult. A recent case was a patient in their 30s who had immediate graft function but heavy proteinuria by day 2 post-living donor transplant and was anuric by day 3. TPE was commenced immediately and continued for many weeks. A biopsy displayed normal light microscopic findings but global podocyte foot process effacement on electron microscopy. He had a complete remission after several worrying weeks. This highlights that recurrent FSGS has a spectrum of presentations from asymptomatic proteinuria to anuria (see case report of primary non-function here).
The data supporting the use of TPE in this setting are limited to case reports and series and has been aggregated in this systematic review of 77 studies including outcome data on 423 patients. The overall rate of remission (proteinuria < 3.5g/day) was 71% with approximately 2/3 of those being complete remissions (<0.5 g/day proteinuria). Remission was more likely in those having treatment commenced within 2 weeks. Age and type of kidney transplant (living /deceased) did not associate with remission. In patients (often children) deemed at high risk for recurrence, an approach sometimes taken is to offer perioperative TPE commencing before transplantation. A retrospective review of 57 consecutive children from Minneapolis, where they started performing TPE in 2006, did not demonstrate any difference in rate of recurrence or time to recurrence with or without TPE.
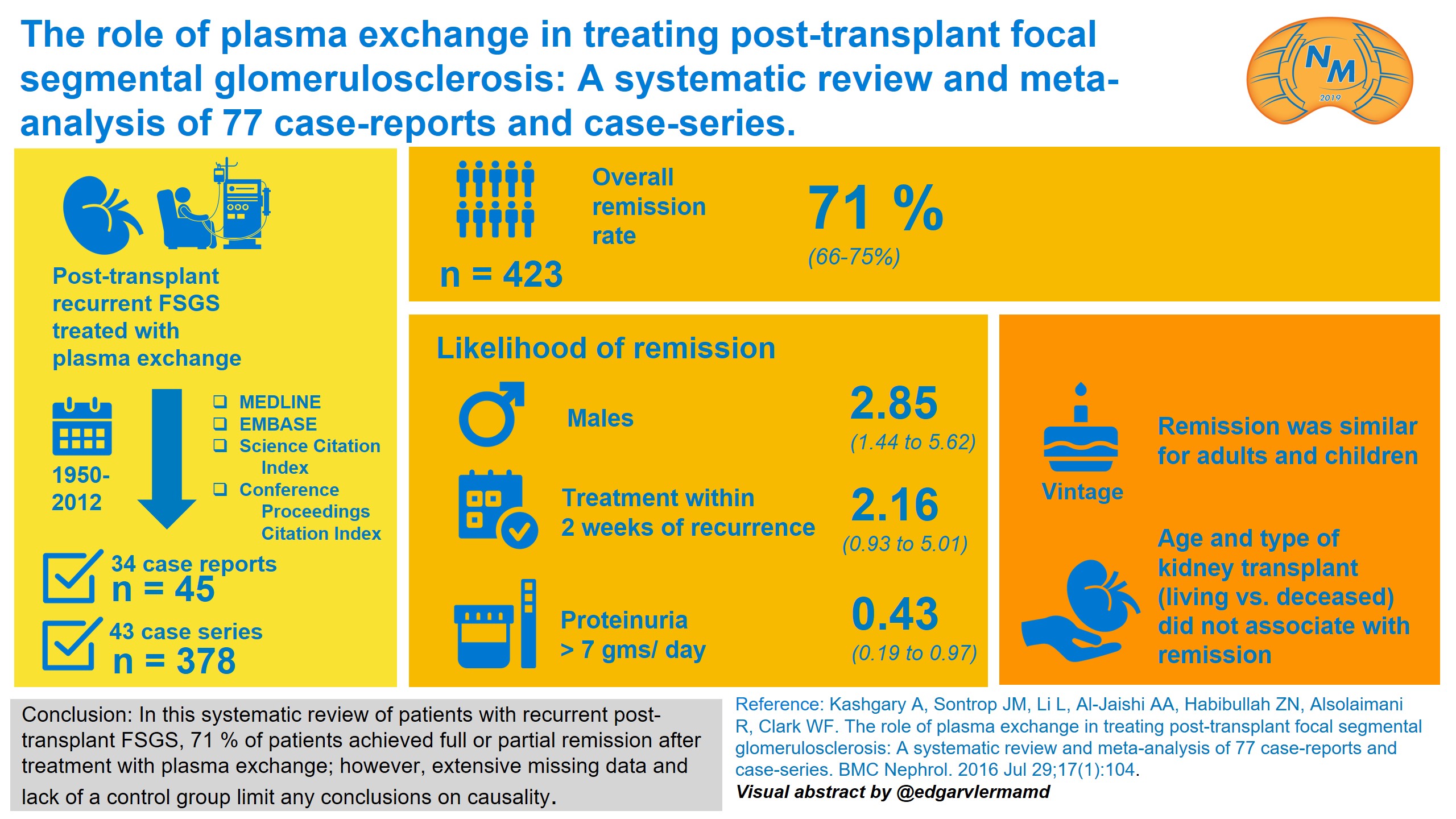
Visual Abstract by @edgarvlermamd on Kashgary et al
Anti-GBM disease
Recurrence of anti-GBM disease post-transplantation is uncommon likely due to maintenance immunosuppression and the practice of delaying transplantation until antibody titers are normal. There is very limited experience with treatment of recurrence given its rarity, although management generally includes TPE as it does for the primary disease. I can find no data on TPE for recurrent anti-GBM disease although we know TPE effectively removes pathogenic anti-GBM antibodies. Even in primary anti-GBM disease, despite the fact we all use it, evidence for the benefit of TPE is limited (here’s a trial with 17 patients from 1985!).
TPE for recurrent disease post-transplant is a journeyman. It’s been around the fringes of the competition for many seasons. It lacks robust supporting evidence and finds itself in a dogfight in this year’s tournament with novel treatments threatening to render it obsolete in certain circumstances.
– Executive Team Member for this region: Timothy Yau, AJKD Social Media Editor. Follow him @Maximal_Change.
How to Claim CME and MOC
US-based physicians can earn 1.0 CME credit and 1.0 MOC point for reading this region.
- Register/log in to the NKF’s Professional Education Resource Center (PERC).
- Review the activity and accreditation information.
- Click “Continue” and review Course Instructions.
- Complete Post-Test. Please note: By selecting “Yes” to the participation questions for each region, the corresponding Post-Test questions will appear. Click “Save Draft” to save your responses and finish later. When you are ready to submit your answers, click “Preview” to review all responses, then click “Submit.”
- Click “Next” to complete the Evaluation form, then click“Submit.”
- Claim 1.0 CME credit and 1.0 MOC point per region (up to 8.0 total for 8 regions of NephMadness).
- Print your certificate.
- Review the Post-Test answers and rationale.
The CME and MOC activity will expire on June 15th, 2019.
Submit your picks! | #NephMadness | @NephMadness | #PLEXRegion
Leave a Reply