
Glomerular Biomarkers – Peering Into the Future
In this author interview, AJKD Social Media Editor, Timothy Yau @Maximal_Change (AJKDBlog), talks to Corey Cavanaugh @cavanaugh_do (CC), co-author of a recent Review article published in AJKD looking at glomerular biomarkers.
AJKDBlog: Let’s start with membranous. We all know the phospholipase A2 receptor (PLA2R) story backwards and forwards by now. But now there are so many other biomarkers like NELL-1 and THSd7A; it’s hard to keep track of all of them now. Can you give us a quick rundown of some of these lesser known proteins?
CC: You aren’t kidding! It’s a wonderful time to be a nephrologist. There is still much more to discover about PLA2R and THSd7A, but since 2019 there have been 6 new antigens/biomarkers discovered including ext1/2, NELL-1, Sema3B, PCDH7, HTRA1, NCAM1. Obviously, information is limited at this stage, but I’ll mention a few clinically relevant things we’ve learned so far.

Intramolecular epitope spreading of the anti–phospholipase A2 receptor antibody (anti-PLA2R) versus baseline multidomain recognition. The reactivity of anti-PLA2R antibodies to a ubiquitous epitope in the cysteine-rich (CysR) domain (left) “spreads” to include subdominant epitopes of the first (center, C-type lectin domain [CTLD1]) and seventh and eighth CTLDs (right, CTLD7 and CTLD8) distinct from the CysR epitope. Disease progression is positively correlated with greater urinary protein excretion and patient age and inversely correlated with the likelihood of remission. An alternative hypothesis is that antibodies to multiple domains are present at the time of diagnosis, and progression of disease is correlated with total anti-PLA2R antibody levels. Abbreviation: FNII, fibronectin type II domain. Figure 1 from Cavanaugh and Okusa, AJKD © National Kidney Foundation
NELL-1 represents likely the 2nd most common antigen in MN, and appears to be highly associated with malignancy, as membranous goes. Think about this antigen when you see segmental capillary loop staining on biopsy and IgG1 is the dominant subclass (remember in primary membranous, IgG4 is the dominant subclass). NELL-1 positivity could inform the provider to pursue a more aggressive search for malignancy in your patient. It’s exciting to know that Nell-1 was also detected in the serum, so hopefully future studies will determine if this can be like PLA2R, and function as a non-invasive biomarker.
Sempha3B seems to represent a biomarker MN in the pediatric population. NCAM1 is a relatively rare antigen in membranous LN, but NCAM1 is also highly expressed in the CNS, potentially linking lupus nephritis and its neuropsychiatric manifestations – I mean, how cool is that? As for PCDH7 and HTRA1 they’re really quite new, and we’ll have to wait for more patients to be studied before drawing and significant conclusions.
To keep reading, in addition to the above articles, check out the the recently published Core Curriculum on membranous nephropathy by Loulwa Alsharhan and Laurence H. Beck, Jr.
AJKDBlog: C3 glomerulopathies are a fascinating group of diseases. We covered genetic and acquired forms of C3GN in NephMadness 2019. Starting with the genetic components like CFB, CFH, CFI, etc – these are the same mutations as seen in atypical HUS. How can mutations in one gene lead to two completely different diseases?
CC: This question has intrigued me as well, and strikes at the heart of how the genotype to phenotype relationship isn’t always predictable. If I’m being honest, there is probably nothing more complicated in nephrology than complement and glomerular disease – so out of respect to some of the brilliant scientists that know a great deal about complement – I’ll try to explain as I understand it (as a clinician).
For a general example, let’s take complement factor H (CFH). CFH is a key soluble regulator of complement, and the N-terminus is responsible for the soluble complement inhibition whereas the C-terminus is responsible for binding C3b on cell surfaces. So, if you have a mutation affecting the N-terminus you get uncontrolled complement activation in the fluid phase (C3GN), but if you have a mutation in the N-terminus you get unprotected endothelial cell surface and thus aHUS. The larger point is that these genes are likely responsible (at least partially) for both diseases because they tend to occur at critical points in the complement cascade, and so it’s not too surprising to see the mutations collect there.
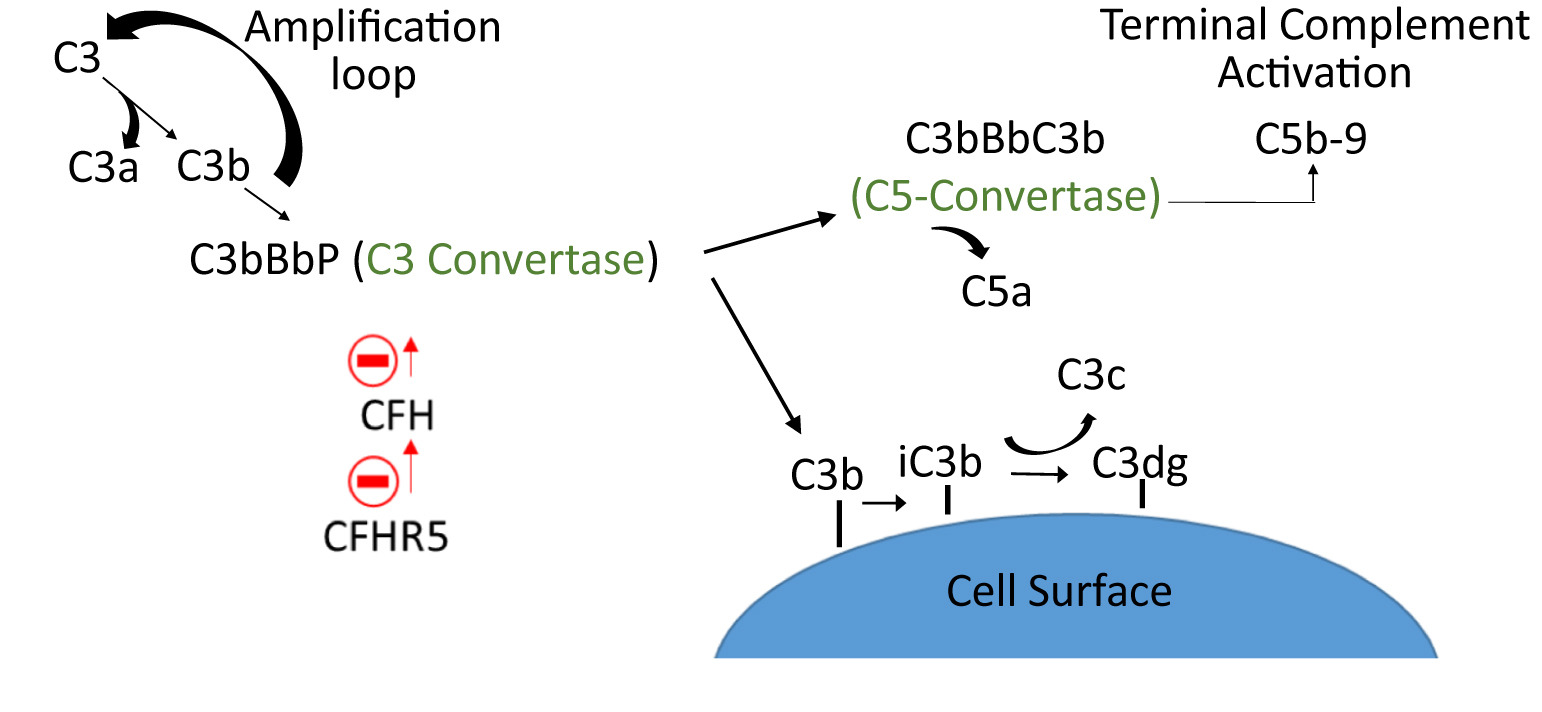
Alternative complement cascade and hypothesized role of complement factor H (CFH)-related protein 5 (CFHR5). Formation of C3 convertases leads to cleavage of C3 and formation of C5 convertase, creating potent anaphylatoxins (C3a and C5a) that mediate the inflammatory response. C3b is degraded into iC3b and C3dg, which mediate phagocytosis and an adaptive immune response. CFH is a strong inhibitor of C3 convertase, whereas CFHR5 preserves C3 convertase activity by inhibiting CFH. C5b causes terminal complement activation membrane attack complexes. Figure 3 from Cavanaugh and Okusa, AJKD © National Kidney Foundation
AJKDBlog: Moving to acquired forms of C3GN, can you tell us about C3 nephritic factor a bit more? Most of us are used to interpreting C3 and C4 levels, but this driver remains elusive to many of us.
CC: C3 nephritic factor is one of the oldest glomerular disease biomarkers in existence, and is still somewhat debated if it is cause vs consequence. I’ll side with the former, but I do not think this disease can be understood by one or two assays – and my recommendation would be to send off a dedicated C3G panel of biomarkers (C5b-9, FB, FH, FI etc), genetic and functional assessment and have an expert help interpret the findings. Complement is only getting more nuanced it seems, and as new therapies are available patient selection will be critical.
For the clinical nephrologist at the bedside, a paraproteinemia assessment is extremely important. In the Mayo clinic study of 114 patients retrospectively studied with C3GN, a majority had monoclonal gammopathy that were 50 years and older. Plus, other studies have shown clone targeted therapy was effective, further suggesting they have a role in complement regulation.
AJKDBlog: Moving from rare to rarer, let’s talk about the update to fibrillary GN. Most fellows know that it is a Congo red negative deposition disease whose organized fibrils are larger (10-30 nm) in diameter than those of amyloid (8-12 nm) but smaller than those of immunotactoid disease (>30 nm). There have even been some reports of Congo red positivity in this disease, so a biomarker that doesn’t rely on us measuring the fibrils by EM is welcome. Tell us about this one.
CC: DNAJB9, put simply, is a big deal. The days of finding and measuring fibrils to clinch the diagnosis in fibrillary GN (FGN) are likely behind us. Along with the reliance on congophilic fibrils, as you point out, it’s not perfect and around 5% of DNAJB9 positive cases were congo red positive. The sensitivity and specificity for immunohistochecmial staining of DNAJB9 approaches 100%. Although determining how DNAJB9 fits into the pathogenesis of FGN still has yet to be fully sorted out, it appears to be the new gold standard of FGN diagnosis.
AJKDBlog: Last random fun question since this was a heavy interview. Your Twitter profile states “Golf/Briskets/GN” as your interests. We’ve talked about GN, and I’m not a golfer. But I recently started doing a lot of home smoking during the pandemic. What are the keys to a good brisket? And is your preference the flat or the point?
CC: Alright, first is to follow Dr. Jay Koyner (@jaykoyner) and the #nephbbq squad on Twitter. The thought of combining nephrologists and BBQ is just too perfect. As for smoking a good brisket, my recommendation is to remember the meat is only as good as the way the animal was raised, so I stick to locally raised, and a local butcher. Ya gotta know what you’re working with. That or wagyu, if you can spend the money. The flat is for sandwiches, the point is for burnt ends (appetizer). Few things in life are better than burnt ends.
To view the Cavanaugh and Okusa review (FREE), please visit AJKD.org.
Title: The Evolving Role of Novel Biomarkers in Glomerular Disease: A Review
Authors: Corey Cavanaugh and Mark D. Okusa
DOI: 10.1053/j.ajkd.2020.06.016
Leave a Reply