
#PathPointer: Casts Give Us Clues – Pigmented Granular Casts on Kidney Biopsy
Tiffany Caza @Tiff_Caza
Dr. Tiffany Caza is a nephropathologist at Arkana Laboratories. She is passionate about kidney disease research and nephropathology education.
In patients with acute tubular injury, characteristics of intratubular casts assist in determining the etiology of disease. Light chain casts have an atypical morphology with a fractured appearance or giant cell reaction, are often PAS-pale, and demonstrate restriction for a single immunoglobulin light chain. Presence of light chain casts is diagnostic of multiple myeloma (a ‘myeloma-defining event’). Red blood cell casts are seen in the setting of an active glomerulonephritis or in anticoagulant-associated nephropathy. White blood cell casts can indicate an ascending infection (i.e. pyelonephritis) or can sometimes be seen in acute interstitial nephritis. Bilirubin casts frequently have a yellow or yellow-green hue on H & E staining and are positive with Hall’s bilirubin stain, where they have a characteristic olive green appearance and are indicative of liver failure (frequently in the setting of hepatorenal syndrome). Hyaline and Tamm-Horsfall protein within casts are PAS-positive and are typically associated with chronic injury. Pigmented granular casts can occur in the setting of myoglobin-cast nephropathy (associated with rhabdomyolysis and myoglobinuria), hemoglobin-cast nephropathy (of which occurs in the setting of intravascular hemolysis and hemoglobinuria), and rarely light chain casts can also have a granular morphology.
To work up a biopsy with pigmented granular casts within tubules, first carefully confirm that there are no light chain restricted casts under routine immunofluorescence. If there is no light chain restriction, immunohistochemical staining for hemoglobin and myoglobin can be instrumental for identifying an underlying etiology. Myoglobin casts are far more common than hemoglobin casts, however, they have indistinguishable morphology and it is recommended to examine both in each case.
Here is a representative biopsy from a patient with acute tubular injury containing pigmented granular casts.
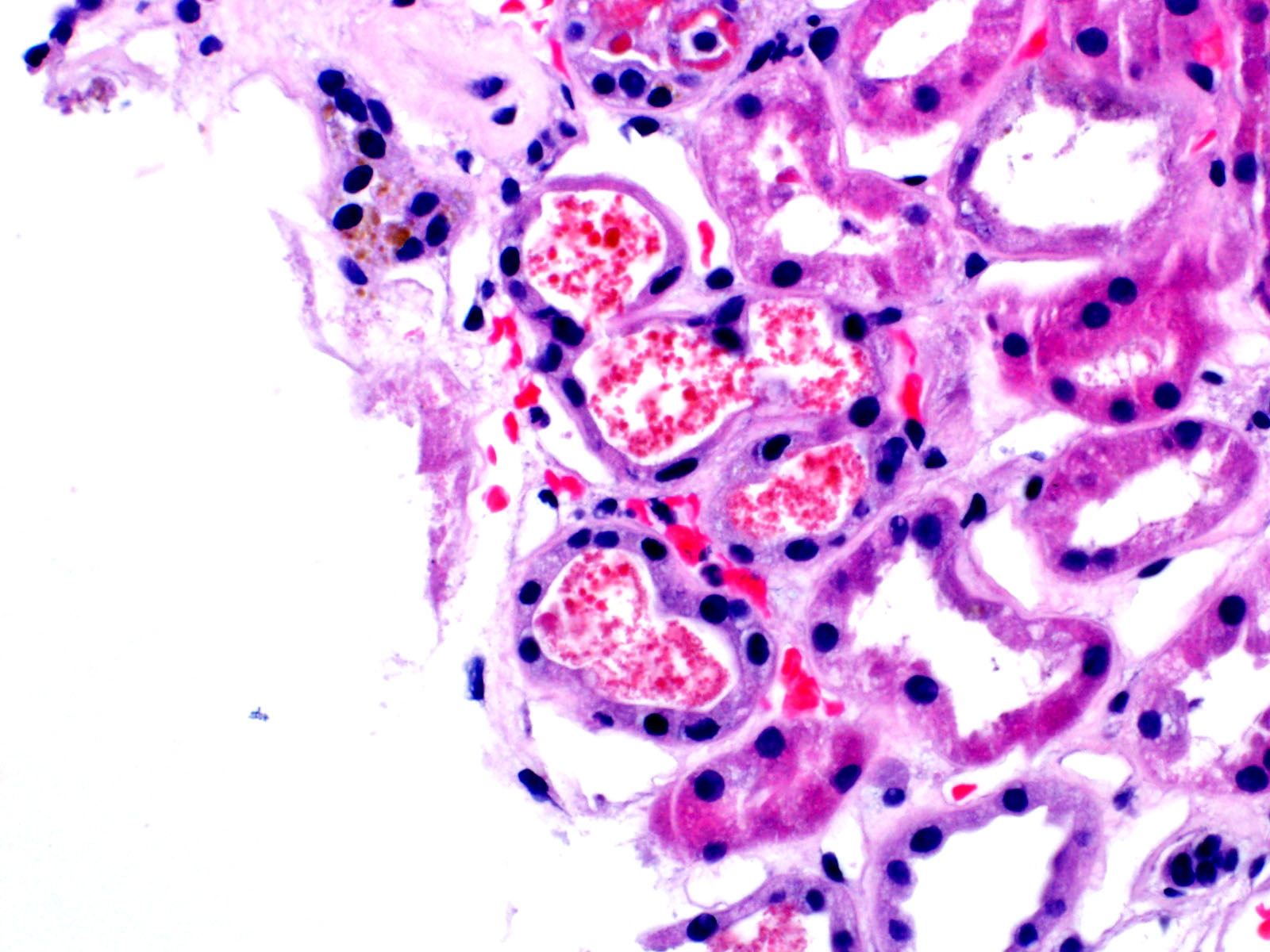
Pigmented granular casts are eosinophilic on H&E staining.

The casts can have a beaded appearance.
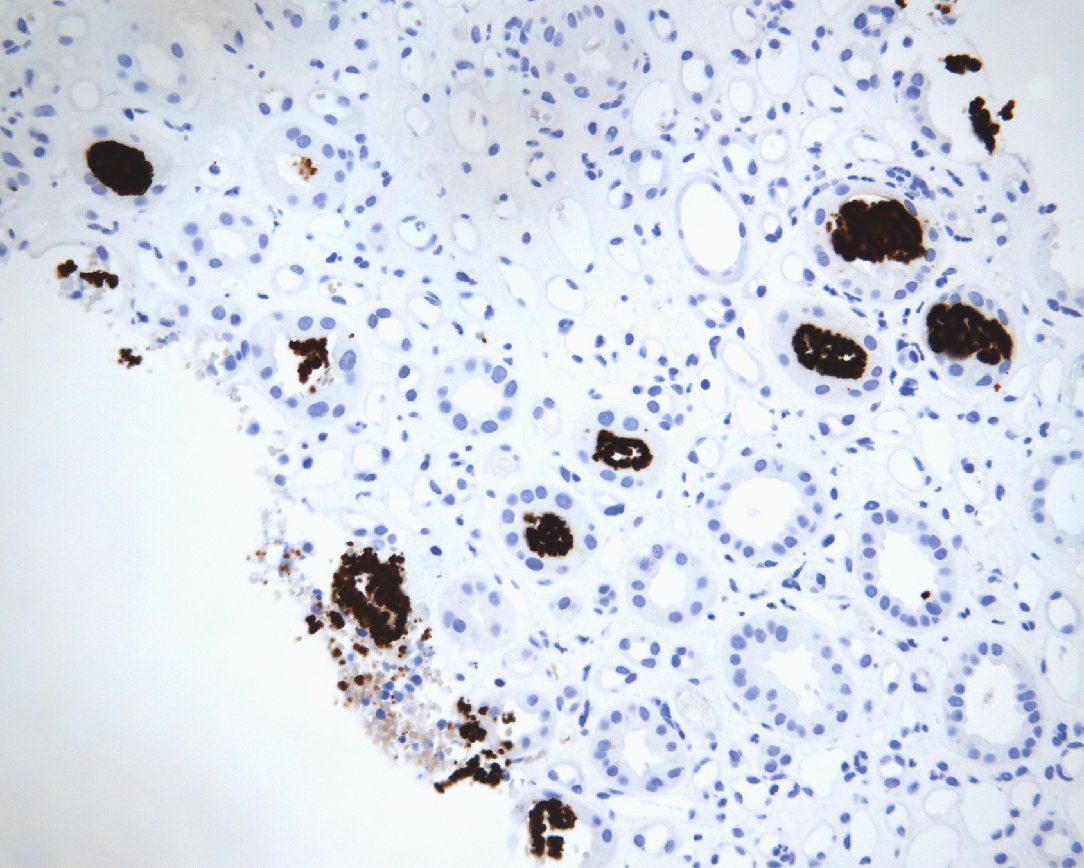
The casts are positive for hemoglobin on immunohistochemical staining. Myoglobin immunohistochemistry is negative (not shown).
The diagnosis in this case is acute tubular injury with hemoglobin casts, or hemolysis-associated hemoglobin cast nephropathy. The presence of hemoglobin casts on a kidney biopsy is highly suspicious for intravascular hemolysis and corresponding hemoglobinuria. In a clinicopathologic case series of 27 patients with hemoglobin cast nephropathy, all patients presented with severe acute kidney injury with a mean creatinine of 8.0 mg/dL. The most common etiologies were medications (especially Rifampin and other antibiotics) and autoimmune hemolytic anemia. Less common etiologies included paroxysmal nocturnal hemoglobinuria, G6PD deficiency, hemolytic transfusion reactions, toxin ingestion, disseminated intravascular coagulation, hemoglobinopathy, snake bites, parasitic infections (such as malaria), and mechanical hemolysis from artificial heart valves.
Myoglobin cast nephropathy, which has an identical morphologic appearance, is 10-fold more common than hemoglobin cast nephropathy. Myoglobin cast nephropathy has an incidence of 0.6-0.8% of all kidney biopsies, with hemoglobin cast nephropathy only 0.063% (Liapis et al, 2016). In a series of 214 patients, acute kidney injury was common with a mean creatinine of 10.8 mg/dL. CPK was markedly elevated in many patients, with the mean CPK of 16,586 IU/mL. The etiologic differential diagnosis is quite broad and includes various sources of muscle injury (seizures, trauma, intense physical activity, surgery), chemotherapy, other drugs (medicinal and illicit), dehydration, sepsis, shock, wasp stings, and snake envenomation.
Acute tubular injury with pigmented granular casts is most frequently caused by hemoglobin or myoglobin cast nephropathy, both of which have a broad etiologic differential diagnosis. Hemoglobin and myoglobin immunohistochemistry is recommended for all kidney biopsies containing pigmented granular or beaded casts to aid in determining an underlying cause.
– Post prepared by Tiffany Caza @Tiff_Caza
Very excellent succinct review