
Glomerulitis Without Evidence of Antibody-Mediated Rejection
PathPointers is a new type of blog post that will highlight important everyday teaching points when reviewing kidney histology. These blog posts will be brief and easy-to-read, using real clinical images to demonstrate various biopsy findings. In addition to AJKD Social Media Editor, Timothy Yau, and Education Editor, Stanley Goldfarb, these posts are also reviewed and edited by Pathology Editor, Matt Palmer.
A kidney transplant patient presenting with rising serum creatinine was subjected to an allograft biopsy. The biopsy showed glomerulitis (Figure 1), a lesion which is typical but not specific for the diagnosis of antibody-mediated rejection (ABMR).

Figure 1. This biopsy shows glomerulitis, which is defined as complete or partial occlusion of one or more glomeruli capillaries by leucocyte infiltration and endothelial-cell enlargement.
In this particular patient, no C4d deposition was seen in the peritubular capillaries, and testing for donor-specific antibodies was also negative. However, careful examination showed viral inclusions (Figure 2), which were subsequently found to stain for cytomegalovirus antigens (Figure 3). Plasma PCR for cytomegalovirus was also positive.
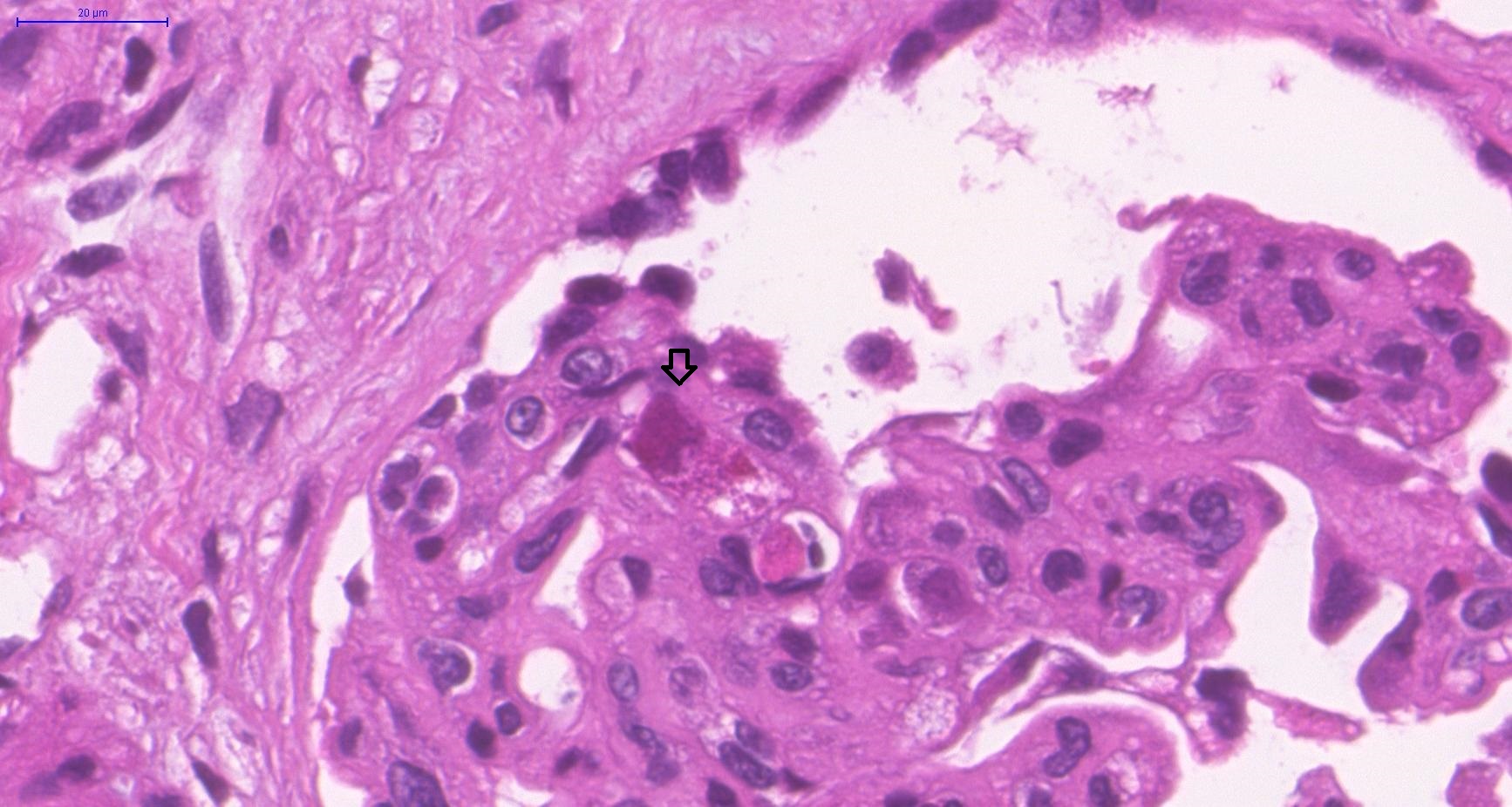
Figure 2. One of the enlarged capillary endothelial cells shows an intra-nuclear inclusion filling up the nucleus. The cytoplasm contains multiple inclusions, all of which represent clusters of replicating viral particles.
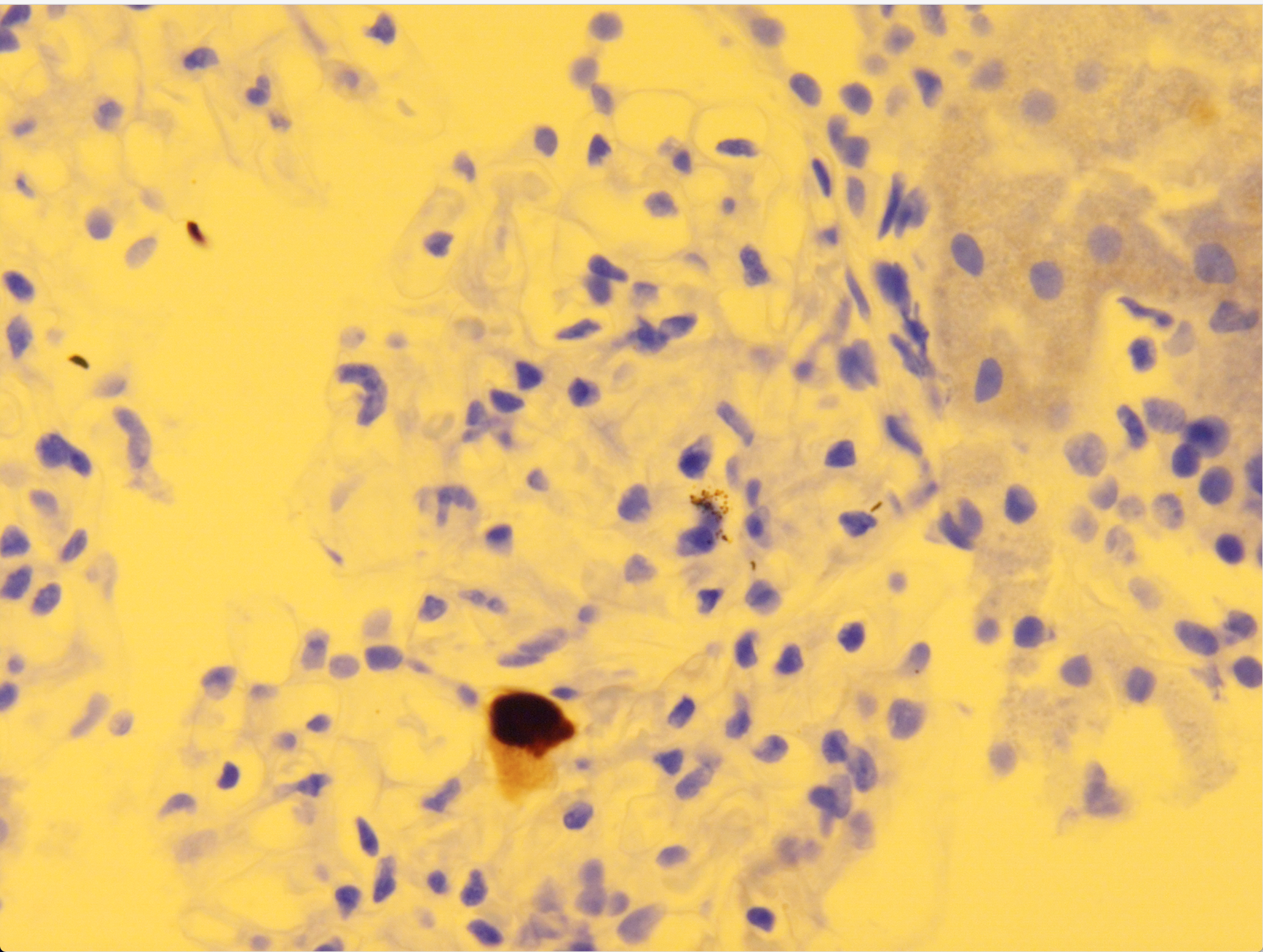
Figure 3. Immunohistochemical stain confirming the presence of CMV-infected cells in this biopsy.
This case illustrates the need to keep a wide differential diagnosis in mind when biopsies with glomerulitis are encountered. While evidence of ABMR will indeed be found in approximately 80% of cases, some cases will not fit the diagnostic criteria. T-cell mediated glomerular endothelial injury, membranoproliferative glomerulonephritis, thrombotic microangiopathy associated with calcineurin inhibitor toxicity, and viral infections will account for a proportion of these cases.
Laboratory workup should include testing for non-HLA donor-specific antibodies, viral PCR, and immunofluorescence, as well as electron microscopic workup for immune complex deposits. DNA microarray analysis (so-called “molecular microscope”) can help in the diagnosis of some C4d-negative cases of ABMR, but molecular results should not override clinical considerations, as the performance of this test in the presence of viral glomerulitis and immune complex glomerulonephritis has not been rigorously examined.
– Post prepared by Parmjeet Randhawa, AJKDBlog Contributor.
Leave a Reply