
#PathPointer: Crescents – A Spectrum of Diseases
PathPointers highlight important everyday teaching points when reviewing kidney histology. These brief and easy-to-read blog posts include real clinical images to demonstrate various biopsy findings.
In this PathPointer I’d like to highlight one of the most worrisome findings one can find on a kidney biopsy: The Crescent.
Most trainees associate crescents with diseases like ANCA vasculitis or anti-GBM disease. Although they are one of many findings that can be seen in these diseases, crescents can be seen in nearly any glomerular process. Even reports of crescent formation in diabetic nephropathy have been reported.
To understand crescent formation, we need to define it and consider the inciting event. A glomerular crescent is cellular proliferation in Bowman’s space that is at least two cell layers thick (cellular crescent). As crescents evolve in the scarring process, they become a mix of cells and collagen (fibrocellular crescent), and later predominantly collagen deposition (fibrous crescent). The mechanisms underlying crescent formation remain poorly understood, but likely involve injury to the glomerular capillary wall, rupture of the basement membrane, and spillage of blood elements like plasma proteins and even cells into the urinary space.
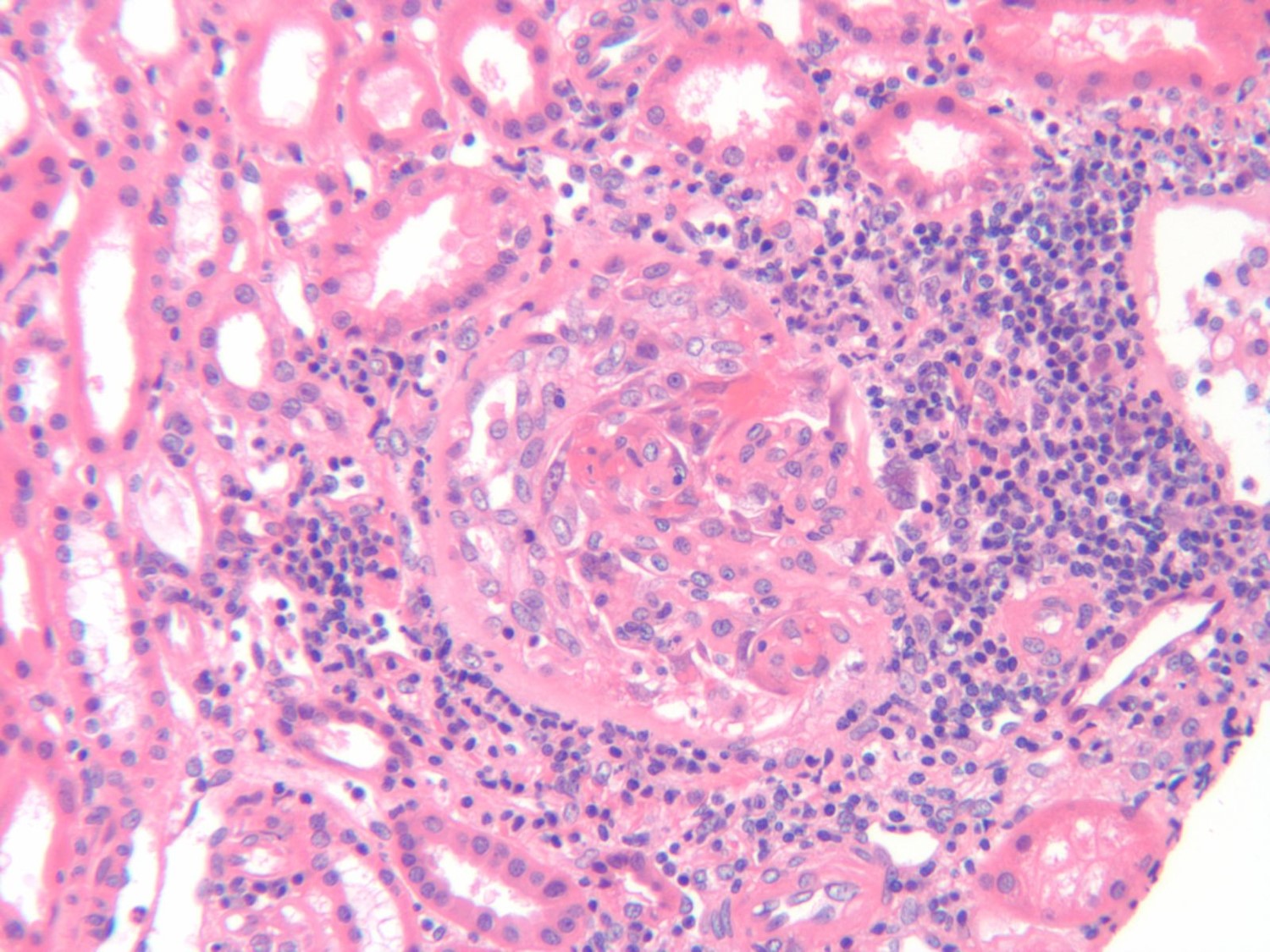
Fig 1. H & E stain of a glomerulus. The crescent is from 6 o’clock to 1 o’clock and is composed of a cellular proliferation with focal fibrin deposition (1 o’clock) that appears to compress the glomerular tuft.
When considering the etiology of a patient with crescents, I think it is easiest to consider the following question:
“What caused damage to the capillary wall that led it to rupture?”

Fig 2. Jones silver stain of a crescent. The capillary loop in the center screen shows a split which has led to spillage of blood contents into the urine space, with subsequent inflammation, cellular proliferation, and fibrin deposition.
Answering this question leads us to the typical 3 broad categories for crescent formation:
- Immune complexes have deposited in the capillary wall (almost always subendothelial), causing it to rupture. This is the broadest category, and includes diseases like lupus nephritis, post infectious glomerulonephritis, IgA nephropathy, etc.
- There is antibody directed against the basement membrane itself, such as anti-GBM disease.
- There are no immune complexes, or it is weakly positive (pauci-immune). ANCA-associated vasculitis is the typical disease in this category.
To answer the above question requires immunofluorescence, and informs the clinician which of the above categories caused the capillary wall to rupture.

Immunofluorescence of various diseases that can lead to crescents. Left panel demonstrates classic linear IgG staining that would be suggestive of anti-GBM disease. Middle panel demonstrates granular immunoglobulin staining that would be seen in lupus nephritis or IgA nephropathy. Right panel demonstrates very weak staining, that would be pauci-immune, and characteristic of ANCA-associated vasculitis.
This PathPointer hopefully demonstrates a basic concept that all of us should keep in mind when coming across the ominous crescent in a kidney biopsy.
– Post prepared by Timothy Yau, AJKD Social Media Editor. Follow him @Maximal_Change.
Leave a Reply