
#NephMadness 2021: ICU Nephrology Region
Submit your picks! | NephMadness 2021 | #NephMadness | #ICURegion
Selection Committee Member: Ashita Tolwani @luck_urine
Dr. Tolwani is Professor of Medicine at the University of Alabama at Birmingham (UAB). She is also the Director for ICU Nephrology at UAB. Her research interests include acute kidney injury, ICU nephrology, and CRRT, with a focus on citrate anticoagulation.
Writer: Ryann Sohaney @RyannSohaney
Ryann Sohaney is a senior staff nephrologist at Henry Ford Hospital and is currently pursuing a Master of Science in Clinical Research Design and Statistical Analysis through the University of Michigan. Her clinical and research interests include acute kidney injury (AKI) and critical care nephrology, with a particular interest in mitigating adverse health outcomes following AKI. She is a former AJKD Editorial Intern.

Competitors for the ICU Nephrology Region
Dialysis Timing in Surgical ICU vs Dialysis Timing in Pediatric ICU
Dialysis With ECMO vs AKI Etiology With ECMO

Copyright: sfam_photo / Shutterstock
Dialysis Timing in Surgical ICU vs Dialysis Timing in Pediatric ICU
A common dilemma in the intensive care unit (ICU) is whether and when to initiate kidney replacement therapy (KRT) for acute kidney injury (AKI). Proponents of an early initiation strategy argue for the potential benefits of avoiding volume overload and maintaining physiologic balance. Conversely, early initiation of KRT may expose patients to an invasive procedure, when kidney function would have otherwise recovered prior to an urgent indication for KRT. There have been several randomized controlled trials to address this issue.
The largest and most recent of these trials, the STandard versus Accelerated initiation of Renal Replacement Therapy (STARRT) AKI was published in 2020. This was a multinational trial randomizing 3,019 critically ill adults with Kidney Disease Improving Global Outcomes (KDIGO) AKI stage 2 or 3 to an accelerated or standard KRT initiation strategy. A serum potassium > 5.5 mEq/L, a serum bicarbonate < 15 mEq/L, or a baseline eGFR < 20 mL/min/1.73m2 were key exclusion criteria. After first meeting inclusion and exclusion criteria, the treating clinician determined clinical equipoise (defined as “the absence of any circumstances that would mandate either immediate initiation of renal-replacement therapy or a deferral of such therapy because of clinical judgment regarding the likelihood of imminent recovery of kidney function”) with respect to the two initiation strategies. Only those for whom clinical equipoise was present were subsequently randomized. Clinicians treating patients in the accelerated strategy were urged to initiate KRT as soon as possible within the first 12 hours of randomization. In the standard strategy arm, clinicians were given the discretion to initiate KRT at any time, although they were provided general indications for initiation, including the following that are refractory to medical management:
- Potassium > 6 meq/L
- pH ≤ 7.2
- Bicarbonate ≤ 12 mEq/L
- PaO2/FiO2 < 200 mmHg plus
- clinical perception of volume overload
- Persistence of kidney injury 72 hours after randomization
There was no difference in the primary outcome of mortality at 90 days (43.9% in accelerated and 43.7% in standard strategy, p = 0.92). Furthermore, survivors of the accelerated strategy were more likely to be KRT-dependent at 90 days or to have experienced an adverse event related to the KRT, suggesting that an early initiation strategy may be associated with harm. Notably, KRT represents a significant escalation in the level of care, as nearly 40% of patients in the standard therapy arm avoided KRT.

Visual abstract by Michelle Lim on STARRT-AKI Investigators et al.
In contrast, is it possible there are populations that may benefit from an accelerated initiation strategy? What clinical parameters do clinicians use when deciding to start KRT? In this scouting report for the ICU Nephrology Region, we draw attention to the current literature and ongoing controversies with respect to initiation of KRT in critically ill surgical and pediatric patients.
Dialysis Timing in Surgical ICU

Copyright: ilikeyellow / Shutterstock
To dialyse or not to dialyse? That is the question often faced by nephrologists caring for surgical patients in the ICU. With over half of surgical ICU patients developing AKI, answering these questions is paramount; When should we initiate KRT? Is high-volume convective clearance necessary? This team will give you the evidence to make the right call for your patient.
An area of increasing attention among surgical patients is perioperative fluid balance. In patients undergoing thoracic surgery, larger intraoperative fluid balance is associated with the development of acute lung injury and mortality. However, the optimal fluid management strategy among critically ill surgical patients continues to be a topic of debate. In a randomized trial of 100 patients undergoing cardiac surgery, researchers reduced ICU length of stay (LOS) and post-operative complications using individualized early goal-directed hemodynamic therapy guided by stroke volume variation, cardiac index, and optimized global end-diastolic volume index. In the control group, hemodynamics were monitored with mean arterial and central venous pressures. Interestingly, there was no difference in the volume of fluids administered between the study arms.
AKI affects almost half of critically ill surgical patients and is associated with increased morbidity and mortality. Optimizing AKI care is thus of critical importance. Does earlier initiation of KRT in critically ill patients with AKI allow for rapid optimization of volume status and lead to improved outcomes? Is there a role for convective clearance to remove inflammatory cytokines?

The HEROICS (High Volume Veno-venous Hemofiltration Versus Standard Care for Post-cardiac Surgery Shock) study, a multicenter randomized trial, enrolled 224 patients with severe shock requiring high dose catecholamines within the first 24 hours post-cardiac surgery. Participants were randomized to either early (within 48 hours of study entry) high volume continuous hemofiltration (80 mL/kg/h) for 48 hours followed by continuous venovenous hemodiafiltration (CVVHDF) or “standard care.” In the standard care arm, CVVHDF (dose < 35 mL/kg/h) was initiated only if creatinine increased > 4 mg/dL or >3 times the preoperative creatinine, urine output < 0.3 mL/kg/h for 24 hours, urea > 36 mmol/L, or if life-threatening hyperkalemia occurred. Participants randomized to high volume hemofiltration experienced shorter duration of catecholamine administration and more rapid resolution in metabolic acidosis. However, there was no difference in ventilator free days, ICU LOS, or survival at 30 days. Similar to prior KRT timing studies, 43% of participants in the standard arm never required KRT. The study was stopped for futility after the enrollment of only two thirds of the intended participants. The results of this study do not support the use of high volume convective and early KRT in patients with shock post-cardiac surgery.
The ELAIN (Early versus late initiation of renal replacement therapy in critically ill patients with acute kidney injury) trial randomized 231 critically ill patients with AKI stage 2 and plasma neutrophil gelatinase-associated lipocalin (NGAL) level greater than 150 ng/mL to either an early (within 8 hours of AKI stage 2) or delayed (within 12 hours of stage 3 AKI) continuous kidney replacement therapy (CKRT) initiation strategy. Almost all patients enrolled in this study were surgical patients. Patients treated with an early initiation strategy experienced lower 90-day mortality, shorter duration of mechanical ventilation, shorter hospital LOS, and greater kidney recovery. A strength of this study was the use of NGAL to enrich the study with participants more likely to experience AKI progression. However, this study is limited by its single-center design. The findings of ELAIN have not been replicated in larger, multi-center trials. For example, a subgroup analysis of nearly 1,000 critically ill surgery patients in STARRT-AKI revealed no difference in all-cause mortality at 90 days.
Defining the optimal time to start KRT based on both observation and trial data is difficult, particularly as the definition of “early” varies across studies. Most nephrologists would agree that the clinical decision to initiate KRT is not based upon serum creatinine values. However, serum creatinine is one of the primary indicators that defines “early” across studies. Trials repeatedly appear to confirm that initiating KRT according to AKI stage is not appropriate and potentially harmful. The potential benefits and harms of initiating KRT versus continued conservative management must be considered for each individual patient, taking into account the current clinical trajectory, comorbid illness, and individual patient goals. Evidence does not currently support that surgical patients — like those with sepsis-associated AKI — are more apt to benefit from earlier and more aggressive application for KRT, although a role for early volume optimization in select patients with suboptimal response to diuretics remains plausible. Future studies may consider moving away from primarily creatinine-based definitions of “early” KRT and seek to implement routine clinical tools, such as the furosemide stress test, to enrich the study population with participants most likely to progress to AKI requiring dialysis (AKI-D).
Dialysis Timing in Pediatric ICU

Copyright: rawf8 / Shutterstock
Fluid overload significantly increases mortality in children admitted to the ICU and providing acute kidney replacement therapy to this population is challenging. How do we overcome these obstacles and provide the best care for our pediatric patients? There are no guidelines for the management of AKI in pediatrics, but this team brings invaluable insight to this area, putting them in position to fight and win the Nephmadness title.
AKI affects 1 in 3 hospitalized children worldwide. Within the ICU, AKI is associated with a mortality of approximately 15% and increases with AKI severity. ICU mortality exceeds 40% in children with AKI requiring KRT. Despite recognition of the adverse health outcomes, there are no pediatric guidelines for the management of AKI. Therefore, with respect to timing of initiation of KRT in critically ill children, pediatric nephrologists and intensivists look to large observational cohorts for clues to guide management.
Fluid overload has repeatedly been associated with adverse health outcomes in critically ill children. Alobaidi and colleagues performed a meta-analysis of studies describing the relationship between fluid overload and various outcomes, revealing a significant association between fluid overload and in-hospital mortality (17 studies, OR 4.34 [95% CI, 3.01-6.26]). In studies assessing fluid overload as a continuous variable, there was a 6% increase in the odds for mortality for every 1% increase in fluid overload per patient (11 studies, adjusted OR 1.06 [95% CI, 1.03-1.10]). Fluid overload was also associated with longer ICU LOS (in 6 studies) and prolonged (> 3 days) mechanical ventilation (in 3 studies).
The Prospective Pediatric CRRT (ppCRRT) Registry is a multicenter, prospective, observational cohort of children treated with CKRT. An analysis of 297 patients from the ppCRRT cohort from 2001-2005 evaluated the relationship between fluid overload at CKRT start and mortality. The degree of fluid overload from time of pediatric ICU admission to CKRT start was determined by:
[(Fluid in [L]- Fluid out [L])/ICU admission weight (kg)] x100
Patients with ≥20% fluid overload at CKRT initiation had 8.5 times the odds of mortality compared to those with fluid overload <20% (95% CI, 2.8 to 25.7) when adjusting for several indicators of severity of illness (including Pediatric Risk of Mortality [PRISM] II score at pediatric ICU admission, multiorgan dysfunction syndrome, oncologic diagnosis, and use of inotropes). In the same study, a multivariable model with fluid overload as a continuous variable demonstrated that the odds of death increased by 3% for every 1% increase in fluid overload (OR 1.03 [95% CI, 1.01-1.05]).

Visual abstract by Divya Bajpai on Sutherland et al.
Findings from the ppCRRT cohort build upon several prior single, center retrospective analyses. In a study of 113 patients receiving continuous venovenous hemofiltration (CVVH), Foland and colleagues demonstrated that fluid overload was a significant predictor of mortality after adjusting for PRISM III score at CVVH initiation (per 10% increase in fluid overload, OR 1.24 [95% CI, 1.02-1.50]). Notably, in children with multiorgan dysfunction syndrome (≥3 organs) only fluid overload (and not PRISM III score) predicted mortality. However, this study also demonstrated that survivors of CVVH had fewer hospital days prior to CVVH initiation (survivors had a median of 3.0 days with interquartile range 1.0-8.0, while non-survivors had a median of 15.5 days with interquartile range 4.0-23.75). The authors attempted to address the potential impact of excess hospital days on fluid overload and mortality by performing several sub analyses. Children with ≥10% fluid overload within 4 days of CVVH initiation were less likely to survive than patients with <10% fluid overload, although there was no difference in survival in patients with 5-7 days of pre-CVVH.
One criticism of these observational analyses is that there may be unmeasured confounders that account for the disparate mortality outcomes between those with and without fluid overload. For example, degree of fluid overload may simply be a marker of severity of illness. Despite the rigor in attempting to address this issue, it remains possible that fluid overload is reactionary to hemodynamic instability and associates with, but is not the underlying cause for mortality. Even still, given the consistent signals from observational data and the lack of clinical equipoise among pediatric nephrologists and intensivists, initiation of KRT to prevent volume overload in children with inadequate response to diuretics is considered a reasonable management strategy.
Compared to adults, provision of acute KRT in children can be more technically challenging. Most hemo circuits used in pediatrics are designed for adults and have a priming volume ranging from 60-170 mL. This can be problematic in infants and small children when priming volume exceeds 10% of blood volume. To mitigate hypotension at CKRT start, blood primers are often required when initiating CKRT in small children. Menon and colleagues described the use of an ultrafiltration device, the Aquadex FlexFlow System, to provide a diverse range of CKRT modalities across multiple institutions. The major advantage of this system is the low extracorporeal volume of 33 mL. Use of this system was described in 46 critically ill neonates, including neonates unable to receive peritoneal dialysis (PD). Overall, modification of the ultrafiltration device for CKRT appeared safe, with access complications accounting for most of the adverse events. This study highlights the ongoing need to develop and implement CKRT devices and protocols specifically for small children and neonates.
A single-center, randomized clinical trial enrolled 73 infants undergoing cardiac surgery with cardiopulmonary bypass experiencing oliguria (urine output <1 mL/kg/h) in the first 4 postoperative hours and randomized these infants to PD or furosemide. Only infants deemed at high risk for AKI preoperatively with a plan to place a PD catheter intraoperatively (per institutional protocol) were enrolled. Infants randomized to PD were managed with a closed-circuit system with initial fill of 10 mL/kg of PD fluid over 5 minutes, dwell of 45 minutes, and passive draining for 10 minutes. This cycle was repeated for the duration of PD. Infants randomized to furosemide were treated with 1 mg/kg every 6 hours for 2 days and then per clinician discretion. Chlorothiazide sodium could be added on postoperative day 2 or later per clinician discretion. Nine of the 41 infants (21%) randomized to PD experienced pleural-peritoneal communication diagnosed via chest tube and did not undergo PD. Eight of the 32 (25%) infants randomized to furosemide had poor urinary response to furosemide, had their PD catheter open to drain, or underwent PD. In an intention-to-treat analysis, there was no difference in the primary outcome of fluid balance on postoperative day 1 between the groups. However, patients randomized to furosemide had 3 times the odds of 10% fluid overload (OR 3.0 [95% CI, 1.3-6.9]) and had 1.5 day longer median duration of inotrope. There was no difference in the median duration of mechanical ventilation between infants randomized to PD vs furosemide. However, infants randomized to furosemide were more likely to require prolonged ventilation (defined post-hoc as greater than 3 days).

Visual abstract by Krithika Mohan on Kwiatkowski et al.
AKI in pediatric patients is life-threatening and the provision of acute KRT in children can be technically challenging. Conveniently, the International Society for Peritoneal Dialysis recently updated their guidelines for PD in AKI in pediatrics. The recommendations guide access and fluid delivery for PD, dialysate solutions for acute PD, the prescription of acute PD, and contains a discussion of continuous flow PD in pediatrics. Importantly, the guidelines state that, “Peritoneal dialysis is a suitable renal replacement therapy modality for treatment of acute kidney injury in children,” giving this recommendation a 1C grade. We are definitely in need of more guidelines and randomized clinical trials to advise optimal therapies in this vulnerable population.
Dialysis With ECMO vs AKI Etiology With ECMO
Dialysis With ECMO
It is only when they go wrong that machines remind you how powerful they are.
– Clive James

Copyright: PIJITRA PHOMKHAM / Shutterstock
Extracorporeal membrane oxygenation (ECMO) is a lifesaving intervention increasingly seen in ICUs. AKI affects more than ⅔ of patients on ECMO. It is therefore crucial that nephrologists caring for critically ill patients on ECMO and requiring dialysis be proficient in their understanding of the ECMO circuit as well as how the ECMO and dialysis circuits are connected.
Extracorporeal membrane oxygenation (ECMO) is a potentially lifesaving intervention for select patients with severe respiratory and/or cardiovascular failure. KDIGO-defined AKI affects nearly 70% of patients with ECMO support, and approximately 40% of patients develop AKI-D while receiving ECMO. With the increasing global utilization of ECMO and the surge of Acute Respiratory Disease Syndrome as a result of the coronavirus pandemic, it is increasingly important for nephrologists caring for critically ill patients to be proficient in the care of patients with AKI receiving ECMO support. In this scouting report, we review the varied etiologies of AKI and the basic principles for providing CKRT during ECMO.
Management of CKRT during ECMO
The objective of venovenous (VV) ECMO is to provide full respiratory support by supplying sufficient oxygenation and removal of carbon dioxide. During VV-ECMO, deoxygenated blood is most often extracted from the vena cava into the ECMO circuit and oxygenated blood is delivered back into the right atrium, thereby decreasing reliance on the lungs for gas exchange.

VV-ECMO, Figure 6A from Griffin et al, AJKD © National Kidney Foundation.
In contrast to VV-ECMO, venoarterial (VA) ECMO provides both respiratory and hemodynamic support. Blood is pumped from the venous system (often the right atrium) and returned to the arterial system (eg the femoral artery), thereby bypassing both the lungs and the heart.

VA-ECMO, Figure 6C from Griffin et al, AJKD © National Kidney Foundation.
Before we dig deeper into this topic, let’s go over the basic anatomy of an ECMO circuit and ECMO terminology:
| Blood pumps | Just as in dialysis, the ECMO circuit requires pumps in order to deliver blood from the patient into the gas exchanger and back to the patient. A typical blood flow for ECMO is 4-6 liters per minute (in adults) and is set by adjusting pump speed (measured in revolutions per minute). |
| Gas Exchange Membrane | The gas exchange membrane, or membrane oxygenator, is responsible for adding oxygen and removing carbon dioxide from the blood, thereby functioning as an artificial lung. As the deoxygenated blood traverses the hollow fibers of the oxygenator, air/oxygen flows in the opposite direction, similar to what is seen in a dialysis countercurrent system with blood and dialysate. |
| Air-Oxygen Mixer | Also called a blender, the air oxygen mixer delivers oxygen to the gas exchange membrane. The fraction of inspired oxygen (FiO2) can be set between 0.21 and 1. The rate that gas is delivered to the gas exchange membrane is referred to as the sweep, and can be set from 0-15 liters per minute. Increasing the sweep increases CO2 removal whereas increasing the FiO2 increases the oxygenation of blood. |
| Heat exchanger | Just as in CKRT, blood in the extracorporeal circuit is exposed to ambient air and must be warmed. A heat exchanger connects to the outflow cannula of the oxygenator to warm the blood to approximately 37 °C before returning it to the patient. |
| Pressure monitors | ECMO circuit pressures are monitored at several locations: venous (inflow) line, pre-oxygenator, and post-oxygenator arterial (outflow/return) line. Increasing ECMO blood flow results in increasingly negative inlet pressure and increasing positive outlet pressure. In adults, an inlet pressure of -100 mmHg and outflow pressure of 300 mmHg is acceptable. The pressure difference across the oxygenator, the transmembrane pressure gradient, represents resistance across the oxygenator. Transmembrane pressure gradients greater than 50 mmHg may suggest the formation of a clot within the oxygenator. |
| Flow sensor | Generally, the flow sensor is positioned to surround the return cannula. This provides insight into how the circuit is functioning. |
| Chugging | Venous collapse may occur due to the negative pressure generated during times of low central venous pressures or high pump speeds. This may be visualized by rhythmic pulsations of the ECMO tubing, referred to as “chugging” or “chatter.” |
Concurrent CKRT and ECMO
Theoretically, all modes of CKRT (CVVH, continuous hemodialysis [CVVHD], CVVHDF, and slow continuous ultrafiltration [SCUF]) can be performed during ECMO, although the requirement for circuit design may vary. During ECMO, CKRT can be delivered by placing a separate CKRT access and running the two circuits independently in-parallel or by incorporating the hemofilter or CKRT circuit into the ECMO circuit. There is no single acceptable method of providing CKRT during ECMO support, and there is considerable variation in practice across ECMO centers.
Delivering CKRT independently from ECMO through a separate access has several advantages. This method allows for the adoption of the hospital’s routine CKRT modality and infrastructure with almost no need for modification. Issues with the CKRT circuit will not interfere with the ECMO circuit and no assistance from the ECMO team is required when making filter or circuit changes. The major downside is the need for an additional large bore access. This can be particularly problematic if the patient was not receiving KRT prior to ECMO cannulation, as systemic anticoagulation is often used during ECMO support. This method also fails to preserve venous access sites should an additional ECMO cannula be required for sufficient ECMO blood flow.
With in-line hemofilters, the filter inlet is connected to a post-blood pump or post-oxygenator and the filter outlet is connected to a pre-blood pump. While this set-up is simple and inexpensive, delivery of effective CKRT may be technically challenging. If dialysate or replacement fluid is being used for solute clearance, separate IV infusion pumps need to be incorporated into the circuit. The rate of ultrafiltration is also set by an IV pump which may be inaccurate. SCUF is the most common in-line hemofilter modality used during ECMO.

CKRT via ECMO. Figure 4 from Van Dyk, released under CC BY-NC-ND 4.0.
Lastly, CKRT can be delivered in-line with the ECMO circuit through the use of a CKRT machine. There are multiple potential configurations, including connecting the CKRT inlet post-blood pump and the CKRT outlet pre-blood pump (via the venous drainage limb of the ECMO circuit). Alternatively, the CKRT inlet and outlet lines can be directly connected to their ports on the oxygenator. The advantages to a CKRT machine in-line approach include being able to take advantage of the CKRT machine pumps, having accurate control of ultrafiltration rate, and having the ability to monitor and respond to changes in transmembrane pressure. However, this comes at the cost of some technical considerations. Connection of the CKRT inlet (arterial access line) post-blood pump results in a positive CKRT access pressure. The venous CKRT return line may also experience higher positive pressures which may require disabling the CKRT pressure alarms using a clamp to control the pressures, or adding additional tubing on both the inlet and outlet lines of the CKRT device.

CKRT circuit to ECMO return line. Figure 5 from Van Dyk, released under CC BY-NC-ND 4.0.
| CKRT-ECMO Circuit | Circuit Design | Advantages | Disadvantages |
| In parallel | CKRT is performed independent of the ECMO circuit through a separate venous catheter | Filter clotting and hemocircuit interruptions do not require assistance from the ECMO team or interfere with the ECMO circuit
Precise control of ultrafiltration rate No restriction in CKRT modality |
Requires an additional venous access, increasing the risk of access complications (bleeding and thrombosis)
The presence of two separate circuits increases extracorporeal blood volume |
| In-line hemofilter | The filter inlet is connected after the ECMO pump or after the oxygenator and returns blood to the proximal portion of the ECMO circuit
Infusion pumps are incorporated into the circuit to control dialysate, replacement and ultrafiltration fluid rates |
Simple and inexpensive | Requires use of several external infusion pumps
Difficult to control ultrafiltration volume Inability to control blood flow rate through the hemofilter No hemofilter pressure monitoring, resulting in diminished ability to detect early filter clotting |
| In-line hemocircuit | Multiple potential circuit configurations:
CKRT circuit connect to luer locks on the inlet and outlet ports of the oxygenator CKRT inlet connected post-blood pump and outlet connect to pre-blood pump (venous drainage limb) |
Precise control of ultrafiltration rate
Ability to monitor transmembrane pressure Does not require external infusions pumps Less priming volume compared to parallel circuit |
May require disabling pressure alarms |
Prevention of circuit clotting
ECMO cannulas and tubing are typically heparin-coated. Despite this, most patients receive systemic unfractionated heparin (UFH) during ECMO to help prevent thrombosis. Much of the time, this may be sufficient to prevent premature clotting of the hemofilter. However, the CKRT circuit is at higher risk of clotting compared to the ECMO circuit due to the smaller diameter and absence of the heparin-coating of the CKRT tubing, as well lower blood flow across the hemofilter. If hemocircuit clotting occurs despite systemic heparin (or if systemic heparin is contraindicated) regional citrate anticoagulation (RCA) can be considered. In a retrospective analysis of 48 consecutive patients undergoing CKRT with the hemocircuit in-line with VV ECMO, Giani et al demonstrated improved clotting-free circuit survival with dual RCA and UFH as compared to UFH alone. Furthermore, there were no occurrences of citrate accumulation. This demonstrates that using RCA and UFH for preventing CKRT hemocircuit clotting during ECMO is safe and effective.

Visual abstract by Sinead Stoneman on Giani et al.
AKI Etiology With ECMO
The news of a good deed travels far, but the news of a bad one travels even farther.
– Polish Proverb

Copyright: Stocksnapper / Shutterstock
“AKI is multifactorial.” How many times did you make that diagnosis following the evaluation of a patient with AKI? In the case of AKI in a patient on ECMO, that statement is very likely to be true. Whether it is hemolysis-associated, or whether it is due to perfusion alterations, one thing is for sure; AKI during ECMO is bad news. And this bad news is planning to travel far into this tournament.
There is wide variability in the reported incidence of AKI during ECMO support, in part, due to the heterogeneity in AKI definitions across studies. In a meta-analysis by Thongprayoon and colleagues, the pooled incidence of AKI across studies was 62.8% (95% confidence interval [CI], 52.1%-72.4%) when consensus definitions of AKI are applied. Moreover, the pooled incidence of AKI-D was 44.9% (95% CI, 40.8%-49.0%). AKI, including AKI-D, was more common among patients supported with VA-ECMO as compared to VV-ECMO. AKI can occur because of the acute illness leading to a need for ECMO, and can be a consequence of the ECMO procedure itself. Before initiation of ECMO, patients may experience AKI from a variety of factors related to the critical illness including sepsis, ischemia (hypotension, use of vasoconstrictive pressors), nephrotoxic medications, and respiratory failure. The initiation of ECMO itself may contribute to the development of AKI through several mechanisms.
Etiology of ECMO-associated AKI
Hemolysis is a common complication of ECMO and can occur as the result of turbulent flow and increased shear force from circuit thrombosis, increased blood pump speeds (roller pump is associated with more hemolysis as compared to centrifugal pump), and high circuit pressures. Free hemoglobin is released during red blood cell destruction and, when severe, saturates the binding capacity of haptoglobin. Plasma free hemoglobin, a marker of hemolysis, is routinely monitored during ECMO. In a single center study by Lyu and colleagues, peak plasma free hemoglobin was a predictor for AKI among patients on VA-ECMO.
Hemolysis can induce acute injury through several broad mechanisms:
- Reduction in kidney blood flow
- Tubular obstruction
- Direct cytotoxicity
Excess free hemoglobin in plasma dissociates from its normal tetramer into a dimer. The hemoglobin dimer sequesters nitric oxide, a potent vasoconstrictor, thereby decreasing kidney perfusion. The dissociation of hemoglobin into a dimer allows it to be filtered through the glomerulus. Free hemoglobin is relatively insoluble in urine and therefore precipitates, forming distal tubular casts that lead to intratubular obstruction.

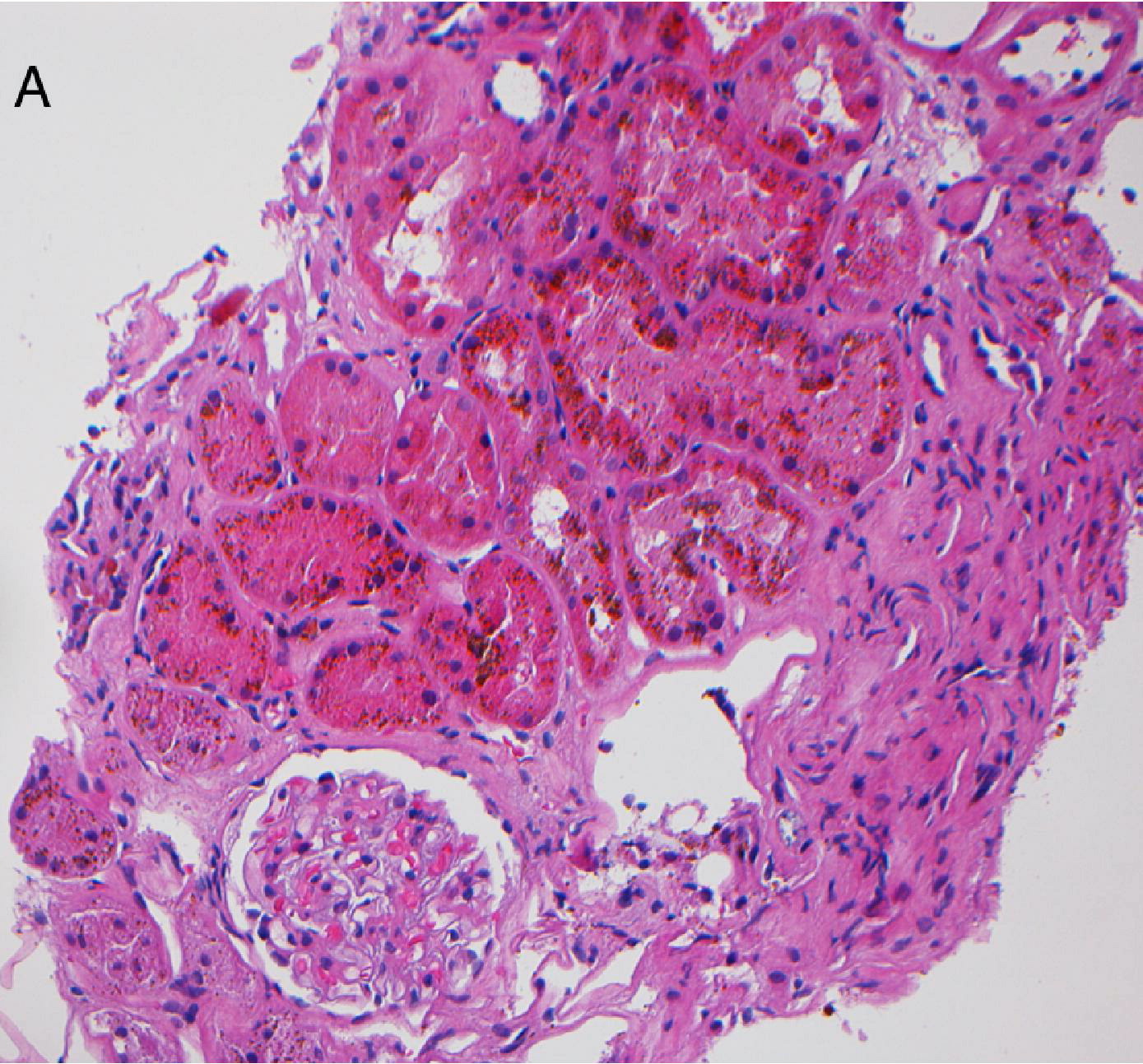
The hemoxylin and eosin stain (panel A) demonstrate distal tubular casts which are periodic acid–Schiff reagent positive (panel B) in a patient with intravascular hemolysis. Figure 1 from Khalighi et al, AJKD © National Kidney Foundation.

Distal tubular casts in a patient with intravascular hemolysis stain strongly positive for hemoglobin A. Figure 2B from Khalighi et al, AJKD © National Kidney Foundation.
Finally, hemoglobin dimers are reabsorbed in the proximal tubule through the megalin-cubilin receptor system. Heme then exerts direct cellular injury through lipid peroxidation, protein oxidation, and injury to mitochondria.
Hematoxylin and eosin stain of kidney tissue with brown pigment deposits in proximal tubular epithelial cells with accompanying tubular degeneration and necrosis. Figure 1A from Qian et al, AJKD © National Kidney Foundation.

Prussian blue iron stain demonstrating that these are hemosiderin deposits with the tubular epithelial cells. Figure 1C from Qian et al, AJKD © National Kidney Foundation.
In addition to hemolysis-associated AKI, ECMO may contribute to AKI through alterations in perfusion and by activation of pro-inflammatory mediators. The exact contribution of these mechanisms to AKI are plausible, but poorly understood. Non-pulsatile perfusion, which occurs during ECMO, increases renin, catecholamine, and vasopressin release. Collectively, these hormonal changes increase vasoconstriction and increase cardiac afterload. Moreover, exposure of blood to the foreign ECMO circuit and shear stress increase the activation of neutrophils and other leukocytes, initiating an inflammatory cascade contributing to multiorgan failure.
AKI and Mortality
Irrespective of the cause, AKI that develops during ECMO support is a major risk factor for mortality. In a meta-analysis including only ECMO studies that adjusted for confounders, there was a 3.3 times greater odds (95% CI, 2.2-5.0) of death among patients with AKI compared to those without. Unfortunately, survival among patients receiving ECMO with AKI does not appear to have improved over time as there was no association between year of study and in-hospital mortality. Perhaps there have been meaningful improvements in the care of patients on ECMO with AKI that are overshadowed by selection of patients for ECMO who are sicker at initiation.
COMMENTARY BY KATHLEEN LIU:
Timing is Everything
– Executive Team Member for this region: Pascale Khairallah, AJKD Editorial Board Member. Follow her @Khairallah_P.
How to Claim CME and MOC
US-based physicians can earn 1.0 CME credit and 1.0 MOC point for reading this region.
- Register/log in to the NKF’s Professional Education Resource Center (PERC). If you select “Physician” in the drop-down menu during registration, the ABIM ID will pop up – make sure to complete this during registration to receive MOC points after course completion.
- Review the activity, disclosure, and accreditation information.
- Click “Continue” and review Course Instructions.
- Complete Post-Test. Please note: By selecting “Yes” to the participation questions for each region, the corresponding Post-Test questions will appear. Click “Save Draft” to save your responses and finish later. When you are ready to submit your answers, click “Preview” to review all responses, then click “Submit.”
- Click “Next” to complete the Evaluation form, then click“Submit.”
- Claim 1.0 CME credit and 1.0 MOC point per region (up to 8.0 total for 8 regions of NephMadness).
- Save/print your certificate.
The CME and MOC activity will expire on June 14th, 2021.
Leave a Reply