
Lymphoma and the Kidney
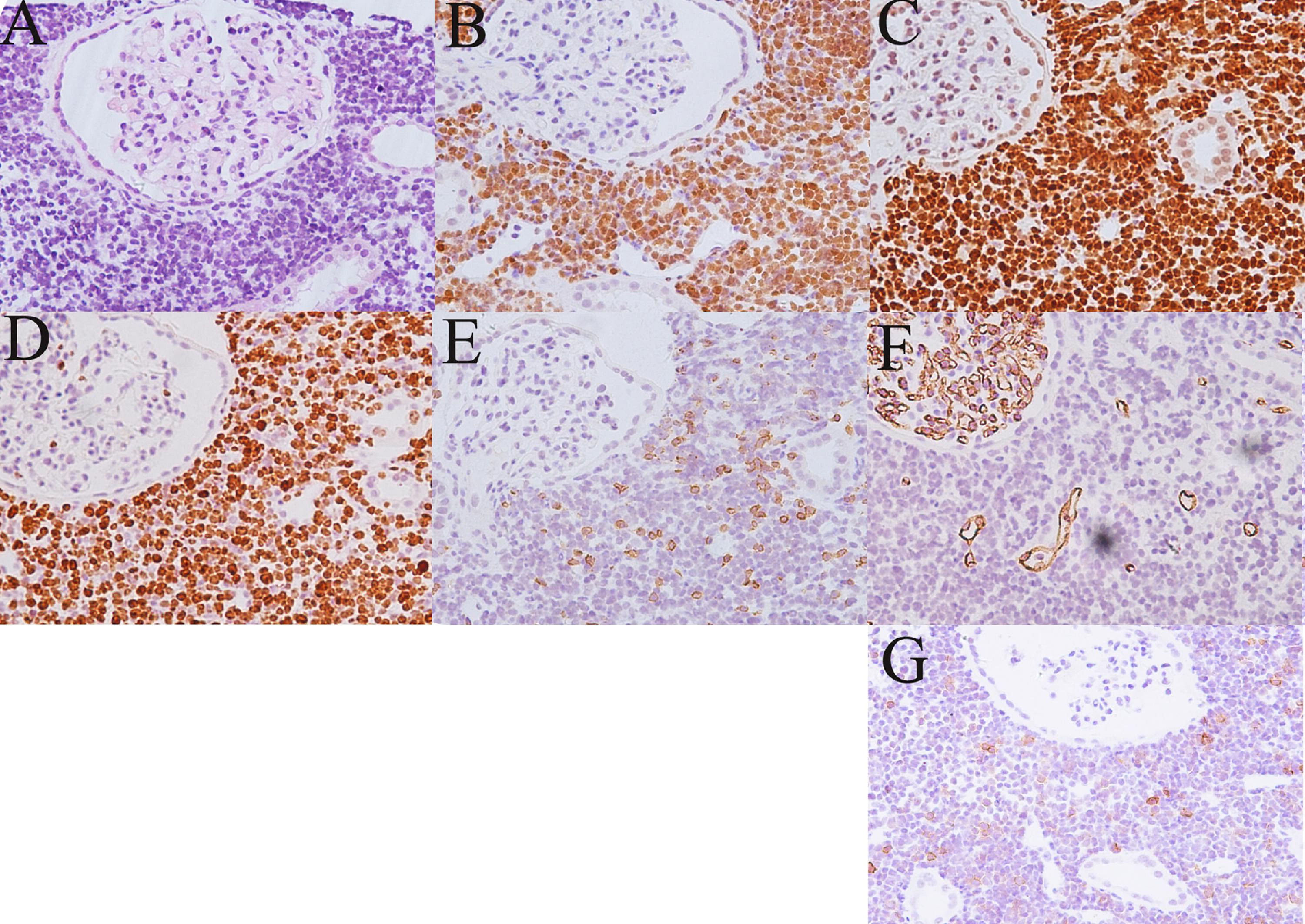
Fig 3 from Shi et al AJKD, © National Kidney Foundation.
Invited commentary by Dr. Parmjeet Randhawa
In the December issue of the American Journal of Kidney Diseases, Shi et al describe a patient with B-cell lymphoma presenting as acute kidney injury (AKI). Lymphomas in the kidney usually present as a mass lesion, typically after the diagnosis of lymphoma has already been established by biopsy of a lymph node or bone marrow. The reported patient is unusual in that the kidney biopsy uncovered the diagnosis for the first time, and that the kidney involvement was bilateral and symmetrical. It is important to keep in mind that the kidney need not be directly infiltrated by lymphoma to result in decreased kidney function. Minimal change disease and nephritic syndrome are well described in patients with both Hodgkin and non-Hodgkin lymphoma. Other cases present as paraprotein deposits in the renal parenchyma.
This interesting case provides an opportunity to describe the spectrum of pathologic findings seen in patients with AKI. The majority of biopsies show non-specific tubular dilatation, loss of brush border, sloughed epithelial cells, apoptosis, and regeneration. A biopsy serves to confirm that the decreased kidney function is tubular in origin, and not due to interstitial nephritis, glomerulonephritis, or vasculitis. The actual etiology of AKI can sometimes be suggested based on histopathologic examination, as in myoglobinuria, hemoglobinuria, and urate or oxalate crystal deposition. For patients presenting with bilateral kidney enlargement, as in this case, the differential diagnosis should include polycystic kidney disease, acute glomerulonephritis, diabetic nephropathy, amyloidosis, metabolic storage diseases, and leukemic infiltration.
Parmjeet Randhawa, MD
Professor of Pathology, University of Pittsburgh Medical Center
AJKD Associate Editor
To view the article abstract or full-text, please visit AJKD.org.
Leave a Reply