
#NephMadness 2020: The Saturated Sixteen
The first round results from NephMadness 2020 are in! Who’s up? Who’s down? Who’s in? Who’s out? Which team was your bracket buster? Where did the Blue Ribbon Panel go wrong? Tweet your reactions with hashtag: #Saturated16
We present the Saturated Sixteen:

Current Standings | Match Results | #NephMadness
Hyperkalemia Region

K is Good in CKD played a strong defense but the strong offensive skills of K Binders in CKD led to a close win.
K Binders in CKD wins 5-4.
Comments from the BRP:
“Interesting and potentially paradigm-shifting concept that higher K associated with better outcomes in CKD.”
“New meds that may allow us to continue renal sparing therapies though currently cost-prohibitive.”
“Most likely to be game-changer in CKD patients; need an alternative to Kayexalate.”
“Since RAASi rocked the word of nephrology (a few years ago…) and since the most common cause of ESRD was/is diabetic nephropathy, and since diabetic nephropathy is so strongly associated with hyporeninemic hypoaldosteronism hyperkalemia, an elevated potassium has been a common limiting factor for the one thing we can do to slow the most common cause of renal failure. Kayexalate is a disaster not just because of the rare colonic necrosis, it is frankly awful to take. The newer K-lowering drugs are game-changers and deserve to win this round. K is good for CKD is a great counterpoint and I love the physiology around the discussion, but it just falls way short and may even be “fake news”. I am craving guacamole now after seeing the picture of the avocados, or maybe just the obligatory margarita that accompanies it. This was an easy call for me.”
“Start the revolution. Your grandmother was right. Eat your fruits and vegetables.”
Team Exercise Causes HyperK was asleep for most of the game, letting team Exercise Prevents HyperK run the court and win in a landslide.
Exercise Prevents HyperK wins 7-2.
Comments from the BRP:
“Exercise is healthy. Don’t argue with me.”
“‘In fact, during short bursts of exhaustive sprinting, arterial potassium concentrations rose by 4.3±0.2 mmol/L, leading to a near doubling in potassium!’ Well, since athletes are not dropping dead (very commonly) while training, this must not be very clinically relevant. The argument for exercise being good for K is compelling. How can you ever vote against exercise for anyone, much less this population of sedentary patients. Another easy call for me.”
“Some evidence that intradialytic exercise reduces potassium rebound post-dialysis.”
“Convincing data plus many other benefits to exercise.”
HD Access Region
Surgical AVF Creation took an early lead but then newcomer Percutaneous AVF Creation’s shots all started falling leading to a solid win.
Percutaneous AVF Creation wins 6-3.
Comments from the BRP:
“Innovative promising technology that benefits selected patients”
“Nothing changed in AVF surgery since Brescia-Cimino AVF – and now after 50 years…this is a game-changer in not only technique/patient comfort but also adding more potential options than the basic few for AV access.”
“It is time to be more progressive in our approach.”
“I am well aware of the pAVF bandwagon frenzy. The technology is amazing as are the videos showing how the two procedures are done. They make it look like a PICC line placement; it is not. The published success results are amazing, but what needs to be stressed is that these results are on highly selected patients. Not everyone is a pAVF candidate, hardly. And this is a relatively new technique. I love, love, love new ideas and questioning conventional wisdom, and especially new technology, but I’m not sure that the pAVF has the gravitas yet. There is nothing like a good old fashioned surgical AVF. The surgery to create one really isn’t that bad compared to a AVG. This was a hard decision because I AM enamored by technology, but I’m sticking with the ‘tired and true’ for now, the surgical AVF. I suspect my BRP colleagues will disagree with me.”
“Magnets are cool!”
“Results appear to be comparable. Success rate is higher, maturation quicker, appearance makes percutaneous the wave of the future. Patients certainly desperately desire it.”
This game was predicted to be a close matchup but in the end, European Guidelines just couldn’t keep up with American Guidelines.
American Guidelines wins 7-2.
Comments from the BRP:
“Details over simplicity. I also like the idea of the ESKD life-plan from American Guidelines.”
“I like that they discuss the ‘evil’ catheter in the American Guidelines.”
“Flipped a coin here, once I woke up from the coma induced by reading this section (no fault to @hswapnil for the excellent writeup, it is the topic!). Heads for EU, tails for US. Heads it was. Sorry for the irresponsible BRP vote this one time.”
“I practice in the US…American Guidelines it is.”
Vaccines Region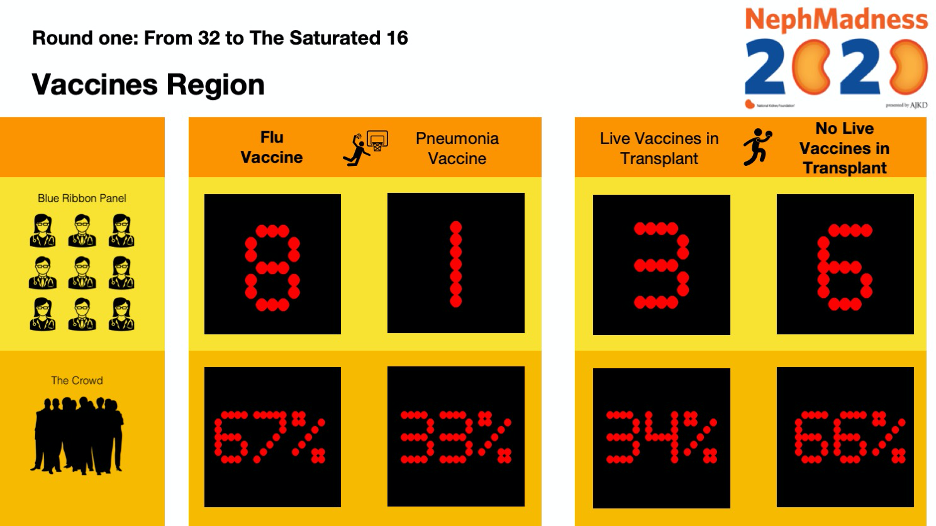
Flu Vaccine dominated on both ends of the court leading to an easy victory over Pneumonia Vaccine.
Flu Vaccine wins 8-1.
Comments from the BRP:
“Very important to reduce seasonal flu prevalence to free up resources for COVID-19.”
“Tough choice – will go with the flu vaccine (high dose vs standard dose).”
“More common disease – I wish there was a coronavirus vaccine! Voting for flu vaccine.”
“Yeesh… this was tough. Figure 4 is amazing. I think the flu vaccine wins by a strand of DNA.”
“Flu vaccine is one of the most cost effective interventions to prevent mortality in CKD.”
Live Vaccines in Transplant played their best game, but it just wasn’t enough to keep up with No Live Vaccines in Transplant.
No Live Vaccines in Transplant wins 6-3.
Comments from the BRP:
“Better to be safe than cause problems in this case.”
“I do not manage transplant patients so I don’t have a practice bias. This may or may not help me on this one. Maybe ‘do no harm’ wins? Live vaccines just seem scary. I have no idea how the rest of the BRP will vote on this one.”
“Compelling insights on both sides but skipping the live vaccines won this one.”
Ethics Region
Coming into this game, Policy-Driven Outcomes for Dialysis had been hot from the 3-point line making them the early favorite. However, the 3-pointers just weren’t falling and Patient-Driven Choice for Dialysis came up with the big win.
Patient-Driven Choice for Dialysis wins 7-2.
Comments from the BRP:
“This is an easy one for me – it has to be patient-centered choice.”
“As bad as patients and families often are in their ESKD decisions, policy mandates are just too slippery a slope in the world we live in, at least in the USA.”
“It is critical that we consider patient choice.”
“Struggled with this one…”
“Policy should catch up to patient-driven outcomes (i.e. home dialysis vs in center hemo). Unfortunately, many policy decisions are made on non-evidence-based factors.”
Dialysis for Patients at End-of-Life could not keep up with End-of-Life Care for Patients on Dialysis’ fast paced offence and strong defense.
End-of-Life Care for Patients on Dialysis wins 7-2.
Comments from the BRP:
“‘Beneficence’/’nonmaleficence’… I’m confused. This has #BlueRibbonFail written all over it.”
“More choices for patients on dialysis.”
“Intriguing data and arguments on both sides. EOL HD argument gave most patient-centered perspective/data.”
“Shared decision-making is essential. Patients are vulnerable and can be persuaded by those focusing on financial factors.”
Green Nephrology Region
Climate Change and AKI and Climate Change and CKD played a close game going into double overtime. But in the end, Climate Change and CKD won out with a last second layup.
Climate Change and CKD wins 5-4.
Comments from the BRP:
“Data support a greater impact on AKI – still unclear about cause of CKDu.”
“Nice topic choice! While I find Meso-American Nephropathy (now described in may other parts of the world) absolutely fascinating, I just cannot believe it is the temperature. Humans evolved in the savannas of Africa. It is toxin(s). The increase in AKI related to global warming, I believe, is real. I suspect the BRP will vote the opposite because of the popularity of that topic in the literature.”
“Insidious and recurrent AKI leads to CKD.”
Consumable Waste in HD came out strong and played like the 2-seed they are, easily beating Disposable Waste in HD.
Consumable Waste in HD wins 7-2.
Comments from the BRP:
“Plastic is recyclable and I see no reason why the dialysis disposables cannot be made into park benches, plastic decking etc. Spent dialysate (WATER) needs to be recycled. Water water water. People have proposed “buddy dialysis” to avoid the need for dialysate in water! If that can even be considered, it tells me that water is the issue here.”
“Mind blown.”
Transplantation Region
Too many fouls by Biopsy in Rejection and a strong showing by Biomarkers in Rejection from the free-throw line led to victory for the latter.
Biomarkers in Rejection wins 6-3.
Comments from the BRP:
“Biomarkers are likely to be more widely used in the short-term.”
“The biopsy is still a more reliable way of making the diagnosis and learning more about the disease.”
“Biomarkers may be the future of all medicine, but they cannot replace a biopsy, at least for now.”
“Eventually, the biopsy will be rarely used.”
A last-minute 3-point shot hitting nothing but net led to a one-point victory for Marijuana is OK in Transplant over Marijuana is Not OK in Transplant.
Marijuana is OK in Transplant wins 5-4.
Comments from the BRP:
“Not enough data to say OK.”
“Some interesting health effects but, like most things, it must be used modestly.”
“Patients will smoke weed. You can ban it and they will lie and pass your tests, or you can know about it and plan accordingly. It is not the devil drug. Do we screen and make decisions for casual alcohol use? Easy call here.”
“Helps ease anxiety faced by patients with CKD…”
Genetics Region
Women with X-Linked Alport took an early lead against Autosomal Dominant Alport and never decreased the pressure leading to a major blowout.
Women with X-Linked Alport wins 7-2.
Comments from the BRP:
“Alport is one of the few situations in life that women get an automatic advantage. But let’s not ignore them entirely. Another easy call.”
“A tough one.”
“Your discussion convinced me Autosomal Dominant Alport is more common than once thought.”
Genetic Counseling for Stones and Genetic Counseling for Cystic Diseases came into this matchup closely matched. Genetic Counseling for Cystic Diseases eked out a victory with a solid defense.
Genetic Counseling for Cystic Diseases wins 5-4.
Comments from the BRP:
“More common disease and now there is treatment (I hope).” – (Genetic Counseling for Cystic Diseases)
“Stones are physiologically fascinating but clinically boring.” (Genetic Counseling for Cystic Diseases)
“Underutilized.” (Genetic Counseling for Stones)
SGLT2i Region
The most watched matchup of the first round was not a disappointment. In a battle of two high octane offenses, TG Feedback scraped out the win over Non-TG Feedback!
TG Feedback wins 5-4.
Comments from the BRP:
“Recent experimental data support this plus it plays into my strong belief in hyperfiltration causing injury (see Kidokoro et al).”
“Occam v Hickam! The NSAID argument makes me think this is much more than TG feedback.”
“It all goes back to the hunter-gatherer days when we did not eat for days.”
“Team Hickam’s Dictum”
There was no contest in the second matchup of this region. SGLT2i Without DM coasted to an easy victory over team SGLT2i in Transplant.
SGLT2i Without DM wins 7-2.
Comments from the BRP:
“I worry about the added effect of CNI induces afferent constriction plus I believe in hyperfiltration as a pathogenic factor in most chronic progressive kidney diseases.”
“How cool would that be if this works in non-diabetics. Easy call.”
“An answer to obesity.”
Current Standings | #NephMadness | @NephMadness | #SaturatedSixteen

How to Claim CME and MOC
US-based physicians can earn 1.0 CME credit and 1.0 MOC point for reading this region.
- Register/log in to the NKF’s Professional Education Resource Center (PERC). If you select “Physician” in the drop-down menu during registration, the ABIM ID will pop up – make sure to complete this during registration to receive MOC points after course completion.
- Review the activity, disclosure, and accreditation information.
- Click “Continue” and review Course Instructions.
- Complete Post-Test. Please note: By selecting “Yes” to the participation questions for each region, the corresponding Post-Test questions will appear. Click “Save Draft” to save your responses and finish later. When you are ready to submit your answers, click “Preview” to review all responses, then click “Submit.”
- Click “Next” to complete the Evaluation form, then click“Submit.”
- Claim 1.0 CME credit and 1.0 MOC point per region (up to 8.0 total for 8 regions of NephMadness).
- Save/print your certificate.
The CME and MOC activity will expire on June 13th, 2020.
Leave a Reply