
HCV D+/R- Kidney Transplantation in the Real-World: Is It Time?
The emergence of direct acting antiviral (DAA) therapy for hepatitis C (HCV) has arguably been one of the most exciting developments in kidney transplantation in the United States this past decade. In 2017, I wrote a 2-part blog on the HCV and kidney transplantation, focusing on the past and present in one blog post, and the future in the other. Just a few short years later, the future appears to be here!
In 2017 and 2018, the pilot studies THINKER and EXPANDER-1 introduced the practice of transplanting kidneys from donors infected with HCV (HCV D+) into uninfected recipients (HCV R-). By utilizing pre-emptive or early treatment initiation with DAA’s and a 12-week course of therapy, all recipients in these studies (N=30) were either cured of HCV or (in a few patients) HCV was not transmitted at all. Kidney function at 6 (EXPANDER-1) and 12 months (THINKER-2) was excellent and there were no major adverse events. In 2020, two other studies performed in a clinical trial setting were published, showing similar results. The table below summarizes these studies.

Abbreviations – DAA (direct acting antivirals), SVR-12 (sustained viral response at 12 weeks)
Research versus Real-World Setting
The promising results from these small clinical trials bring up the question as to whether this data is sufficient to implement HCV D+/R- kidney transplantation in a real-world or “standard of care” setting. Indeed, more than a handful of US transplant programs have adopted this practice outside of clinical trials or research studies. A study examining US registry data from April 2015 to March 2019 found that utilization of HCV+ kidneys increased over the study period, and there was a dramatic increase in the allocation of HCV+ kidneys to HCV- recipients, particularly in the Southeast and Mid-Atlantic United Network for Organ Sharing regions. A survey of US kidney transplant programs found that among 112 programs that responded to the survey (representing 54% of programs in the US), 58% of programs offered HCV D+/R- kidney transplantation and 14% offered this as “standard of care”.
A big difference, however, with HCV D+/R- transplantation in the real-world setting versus in a clinical trial or research setting is that unlike in clinical trials or research studies, DAA therapy is usually not available prior to or early after transplantation unless it is provided (and paid for) by the transplant center. Third-party payers currently do not cover DAA therapy prior to transplantation. Therefore, assuming transplant centers are unwilling to incur the upfront cost of DAA therapy, the order of events are usually to:
- Perform the transplant
- Document recipient HCV viremia and HCV genotype
- Obtain third-party payer approval for DAA, and finally
- Initiate HCV treatment with DAA.
The delay in DAA treatment in this scenario results in sustained recipient HCV viremia for at least a few weeks. Why is this a problem? Two major potential concerns have been raised:
- HCV-induced immunologic activation with a resultant increased risk for acute rejection and infections with CMV and BK, and
- Risk of serious and life-threatening complications such as fibrosing cholestatic hepatitis (FCH).
Additional concerns that have been brought up regarding HCV D+/R- transplantation in the real-world setting include the possibility of denial of DAA coverage by third party payers, and suboptimal oversight with regards to patient education and the consent process.
Last year, Molnar and colleagues reported their single center real-world experience with 53 patients and 6-month outcomes. All patients in their cohort were able to access DAA and achieved SVR-12 after treatment, which is considered a cure. Patients were initiated on DAA therapy at a median of 76 days post-transplant. Among the 53 patients, one patient developed FCH, 60% of patients had documented CMV viremia and 34% of patients had BK viremia. In another single center real-world experience, Kapila and colleagues reported outcomes in 64 kidney transplant recipients. Among the 58 who had started or completed DAA therapy, only one patient did not respond to DAA due to nonstructural protein 5A resistance. The SVR-12 rate remained excellent, at 98%. The median time to initiation of DAA therapy post-transplant in this cohort was 72 days. Importantly, two patients developed FCH and there was one death.
In their current AJKD article, Molnar and colleagues expand on their previous report and include 65 HCV- recipients of HCV+ kidneys in 2018 with 12-month follow-up data, focusing on kidney outcomes. Compared to 59 recipients at their center who received HCV- kidneys in 2018, they found no difference in post-transplant eGFR, acute rejection rates, and development of donor specific antibodies. One patient in the HCV+ group had biopsy-proven BK nephropathy. At 12 months after receipt of HCV+ kidneys, mean eGFR was 64 ml/min/1.73m2. In addition, all patients were able to access DAA and achieve SVR-12. The authors noted an improvement in timeliness to initiation of DAA treatment over the study period, and stated that their center’s current time between transplantation and treatment initiation is approximately 3-4 weeks.
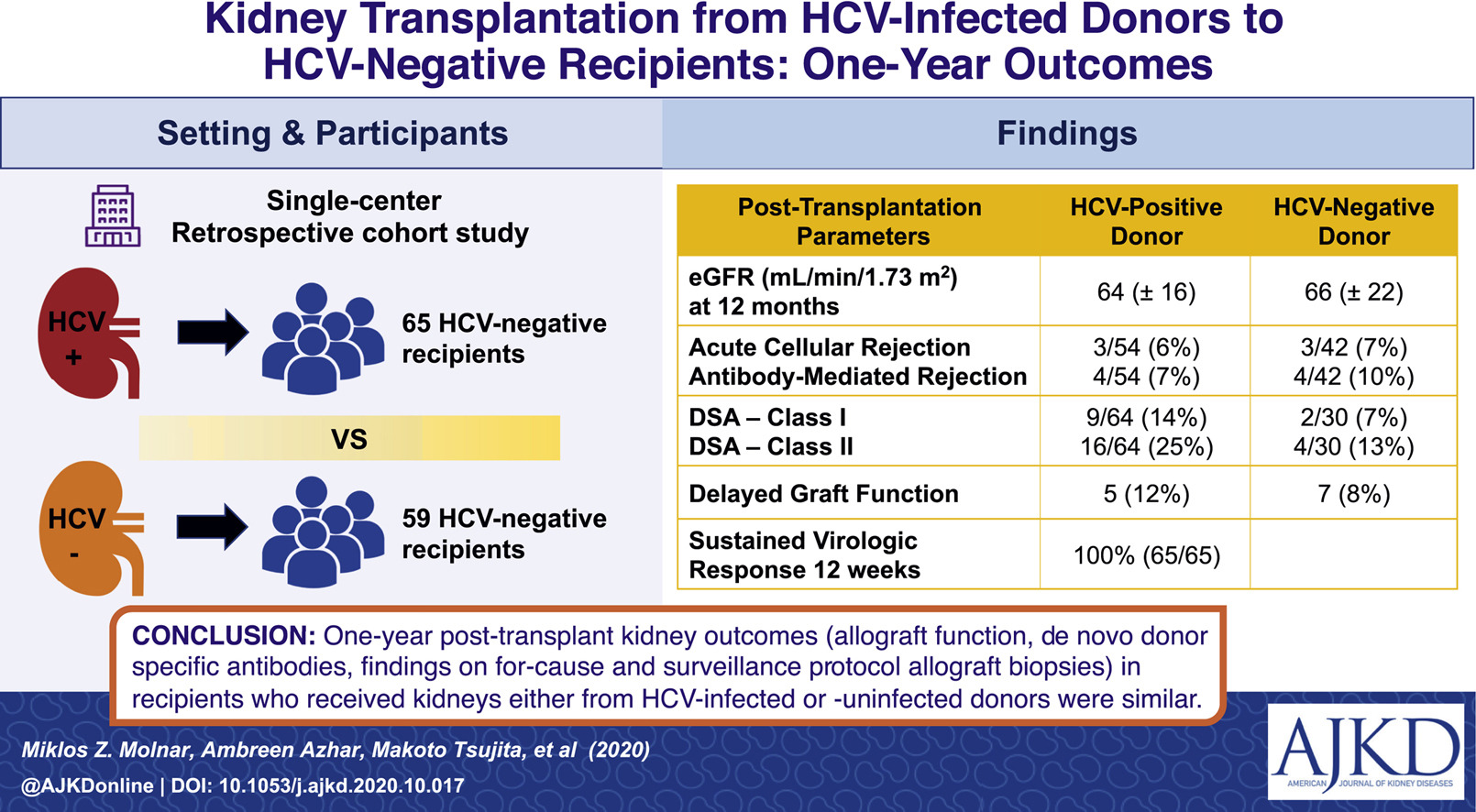
Graphical Abstract from Molnar et al, AJKD © National Kidney Foundation
Do Benefits Outweigh Risks in the Real-World?
Taken together, the published experiences of HCV D+/R- kidney transplantation in a real-world setting are certainly intriguing, and despite the 2 to 3 month delay in initiation of DAA treatment resulting in sustained HCV viremia, the outcomes appear promising. Molnar and colleagues’ current study provides some reassurance regarding the lack of any increased risk of adverse kidney outcomes, including acute rejection and graft loss. However, one must be cognizant that the number of participants in this study remains relatively small and that it carries the limitations of being a retrospective single-center study.
It is easy to say that more data is needed because that is certainly true (more on this later). However, while we await the results of future prospective multi-center studies, is the available data sufficient to continue with this real-world practice? Of course, it boils down to weighing risks versus benefits, and weighing these risks versus “other risks”.
- The strongest “benefit” argument for continuing the practice is that it allows us to maximize the utilization of HCV+ kidneys, help alleviate the organ shortage, and increase access to transplantation for the >90,000 patients waiting on the deceased donor list. There is certainly room for this, as shown in a study of OPTN data which found that in 2019, HCV+ kidneys were still 48% more likely to be discarded compared to HCV- kidneys.
- What about risks? Based on Molnar and colleagues’ experience, the risks appear to be minimal with regards to kidney adverse events. However, there remains a signal for increased rates of CMV and BK infection and the rare possibility of developing FCH (cumulatively, 3 cases have been reported in the literature).
- As mentioned above, the risks associated with HCV D+/R- transplantation in the real-world must also be weighed against “other” risks, specifically those associated with delaying transplantation and prolonging a patient’s waiting time by turning down HCV+ kidneys.
What about the patient perspective on this issue? In a conjoint analysis of 189 kidney transplant candidates conducted at 2 transplant centers where participants were presented with 12 hypothetical decisions about accepting HCV+ kidneys under varying scenarios, participants were more likely to accept a HCV+ kidney with higher cure rates, a younger donor, and a longer waiting time for a HCV- kidney. These are important parameters for transplant programs to consider when discussing risks and benefits with transplant candidates during the consent process and when selecting suitable HCV+ deceased donors.
Alternative Approaches and the Path Forward
It is worth mentioning that preliminary experience on a prophylactic approach to therapy with shorter courses of DAA have also been published? In a single-center pilot trial utilizing pan-genotypic DAA, 10 patients received 1 dose of sofosbuvir/velpatasvir prior to transplant and another dose on postoperative day 1. Meanwhile, 40 patients received 1 dose of sofosbuvir/velpatasvir prior to transplant and 3 additional doses on postoperative days 1, 2 and 3. The overall viral transmission rate was 12%, and was lower with the 4-day strategy, at 7.5%. Those who developed viremia were treated with a 12-week course of DAA. However, 2 patients required a second course of DAA and 1 patient did not achieve SVR-12. In another study, a 4-week course of glecaprevir/brentasvir was administered to 10 patients, with the first dose given prior to transplant. All recipients had undetectable viremia by postoperative day 7. This study makes the argument that perhaps a 4-week (versus 12-week) pre-emptive or “prophylactic” course of DAA therapy is sufficient. This is important because a 4-week course would be less costly, and if outcomes are non-inferior to the standard 8-12 week course of DAA therapy, then transplant centers or third-party payers may be more willing to cover the upfront cost of DAAs prior to transplantation.
Many questions remain. Future studies will need to determine:
- The optimal duration of therapy
- Any differences in outcomes with a preemptive vs early vs delayed DAA treatment strategy
- The risks of CMV and BK infections
- How to optimize patient selection—are there patients who are more likely to benefit (eg, those with expected prolonged waiting time)? Are there those that are more likely to be harmed (eg, those with pre-existing liver disease, older patients)?
In the future, answering these questions and incorporating cost-effectiveness data (previously reviewed in another blog post) will likely form the basis of third-party payer’s approval for DAAs prior to transplantation.
Final Thoughts
The field of HCV and kidney transplantation continues to evolve rapidly. The practice of HCV D+/R- transplantation has been truly innovative, with an immediate and direct impact on numerous patients who have been awaiting transplantation. Efforts should continue to fine-tune this practice, and cumulative experience along with well-designed studies will ultimately allow us to provide our patients with the best possible outcomes.
– Post prepared by Beatrice Concepcion, AJKD Social Media Advisory Board member. Follow her @KidneyBea_n.
To view Molnar et al [subscription required] please visit AJKD.org.
Title: Transplantation of Kidneys From Hepatitis C Virus-Infected Donors to Hepatitis C Virus-Negative Recipients: One-Year Kidney Allograft Outcomes
Authors: Miklos Z. Molnar, Ambreen Azhar, Makoto Tsujita, Manish Talwar, Vasanthi Balaraman, Anshul Bhalla, Pradeep S.B. Podila, Jiten Kothadia, Uchenna A. Agbim, Benedict Maliakkal, Sanjaya K. Satapathy, Csaba P. Kovesdy, Satheesh Nair, James D. Eason
Leave a Reply